INTRODUCTION
Klippel-Feil syndrome (KFS) was first reported by Klippel and Feil in 191210), and is characterized by inappropriate congenital segmentation or fusion of two or more cervical vertebrae4) and exhibits upward translation of upper thorax2). KFS is a mixed anomaly of osseous and visceral developments, with an estimated incidence of approximately 1/42,000 births9). However, the actual prevalence is believed to be higher due to missed diagnoses due to heterogeneity in phenotypic expression15). Common signs of KFS include short neck, low posterior hairline, and restricted mobility of the upper spine, which were manifested in less than 50% of KFS patients15).
Cervical deformity in KFS can cause radiculopathy or myelopathy. Cervical myelopathy represents the most serious complication of KFS, and is usually caused by spinal stenosis at C1 level16). Surgery is indicated in the patients with medically refractory neurological symptoms, which generally involves C1 decompression with craniocervical fixation1,5,8). However, there appears to be no clear evidence regarding the reason for craniocervical fixation in these patients. In the patients without spinal instability, a craniocervical fixation can cause unnecessary motion restriction at the occipito-atlantic and upper cervical joints, the most mobile segment of cervical spine18). It is also unclear whether successful outcomes can be achieved by decompression alone without craniocervical fixation in KFS patients without spinal instability.
Here we report two cases of KFS with C1 myelopathy without C1-2 instability, who received simple decompression without fixation and showed favorable long-term results.
CASE REPORT
Case 1
A 59-year-old male patient was admitted with the chief complaint of hoarseness. The patient was diagnosed as recurrent laryngeal nerve dysfunction due to aneurysmal dilatation of the aortic arch, and graft replacement of aortic arch was performed by thoracic surgery department. Although the patient had features consistent with KFS, there were no spine-related symptoms, neck pain, radiculopathy, or myelopathy before the surgery. During the surgery, the patient was positioned with neck hyperextension. Immediately after recovery from anesthesia, the patient showed motor weaknesses in the bilateral arms and legs, and was subsequently referred to neurosurgery department.
Neurological examination revealed spastic paralysis (grade IV) and Hoffman's sign in the right arm, subjective weakness without pathologic sign in the left arm, and spastic paralysis (grade II) with ankle clonus and Babinski sign in the bilateral legs. Pain and temperature sensation were normal, but proprioception of position, vibration, and light touch were diminished in the bilateral legs.
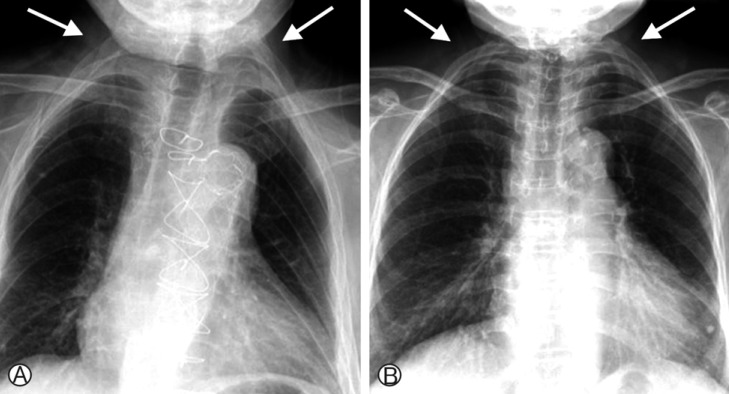
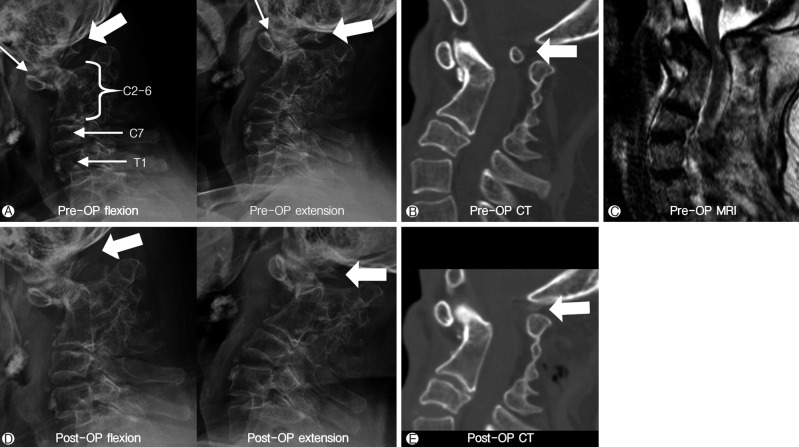
On the chest radiograph, abnormally elevated upper ribs were observed (Fig. 1A). On the cervical radiograph, multilevel fusion was present from C2-C6, and the atlantodental interval (ADI) was 2mm at both flexion and extension lateral views without any spinal instability (Fig. 2A). Computed tomography (CT) confirmed the fused cervical region to be C2-C6. An excessive kyphotic change was noted in the fused segment with forward displacement of C1-2, which resulted in stenosis between kyphotic apex and C1 posterior arch (Fig. 2B). On magnetic resonance imaging (MRI), high signal intensity cord lesion was observed on T2-weighted images between the kyphotic apex and C1 posterior arch mainly at the posterior part of spinal cord (Fig. 2C). The patient's presentation was consistent with Type I KFS (multiple spinal fusions restricted to the cervical vertebrae) according to Feil's classification4), and Type III KFS (multiple contiguous fused segments) according to Samartzis' classification5).
We planned to remove C1 posterior arch which was the primary cause of cord compression, but not to perform craniospinal fixation due to the absence of instability in the C1-2 joint. Immediately after the operation, motor power improved to grade V in the arms and grade IV in the legs. The decreased proprioception in the legs also showed immediate improvement. Physical therapy with active exercise was prescribed postoperatively. The patient was discharged 3 weeks postoperatively with normal gait and muscle power (grade V) in the arms and legs. A soft neck collar was kept for 2 months postoperatively, and patient was checked follow-up dynamic cervical radiography. At 2 years postoperatively, his motor function was well maintained without any new symptom. There was no instability at occiput-C1-2 joints on the cervical spine flexion and extension radiography and CT performed at 2 years after the surgery (Fig. 2 D, E).
Case 2
A 62-year-old female patient was transferred due to acute onset of gait disturbance, radiating pain (VAS 7) in all extremities during admission at gynecological clinic. She also had features consistent with KFS, including a short neck and low posterior hairline. There was a 10-year history of posterior neck pain, occipital hypoesthesia, radiating pain and numbness in all extremities, and subjective gait disturbance. She never visited a hospital for the problems because the symptoms had been mild without any disturbance in the activities of daily living.
Neurological examination revealed normal motor power in the arms. However, there were positive Hoffmann's sign and mild spasticity bilaterally. She had mild paraparesis (grade IV) with spasticity in the legs and showed an unstable gait. Pain and temperature sensation was normal, but proprioception was decreased in the legs bilaterally.
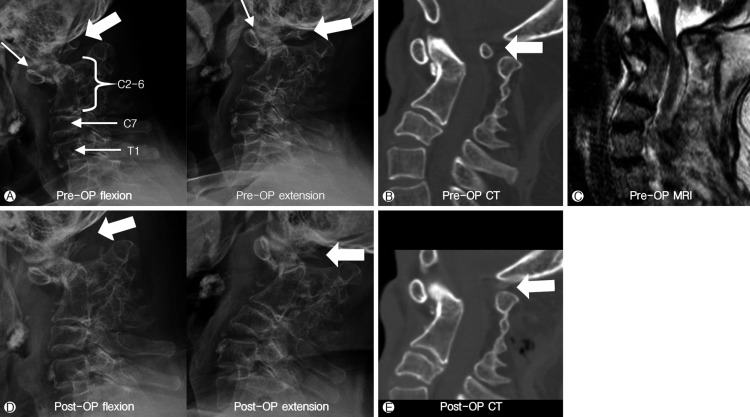
The forms of deformity, stenosis, and cord lesion were similar to those of case 1 on cervical spine radiograph, CT, and MRI (Fig. 3). The ADI was 2.5mm on both flexion and extension lateral views without any definitive craniocervical instability (Fig. 3A). There were stenosis and spinal cord compression by anteriorly displaced C1 arch on preoperative CT and MRI (Fig. 3B, C). The patient's presentation was consistent with Type I KFS according to Feil's classification4), and Type III according to Samartzis' classification5).
We also planned to decompress spinal cord by removing C1 posterior arch without craniocervical fixation (Fig. 3E). In this case, we had to perform suboccipital craniectomy and partial removal of C2 spinous process and lamina in order to make space for the route reaching to the C1 posterior arch (Fig. 3E). Immediately after decompression, there was an improvement in the radiating pain of all extremities (VAS 3), and muscle power recovered to grade V in the legs bilaterally. The unstable gait, spasticity, and proprioception also showed a substantial improvement. Additional physical therapy was not needed, and the patient was discharged at 2 weeks after the surgery without any neurological deficit. A soft neck collar was worn for 2 months postoperatively. Her clinical condition was stable without any craniocervical instability until 2 years after the surgery (Fig. 3D).
DISCUSSION
The characteristic appearance of short neck is known to be associated with several congenital disorders including Turner syndrome, Noonan syndrome, and KFS12). KFS was first reported by Maurice Klippel and André Feil in 1912 as a con- dition of congenital fusion of two or more cervical vertebrae4). KFS is known to have either an autosomal recessive or autosomal dominant pattern of inheritance with mutations in the GDF3 and GDF6 genes19,20). Other features may include a low hairline, neck motion limitation due to cervical fusion, elevated scapula, facial asymmetry, torticollis, and webbed neck15). Spinal abnormalities predominantly occur in the cervical region; however, they may be accompanied by scoliosis or spinal bifida in thoracic or lumbar spine15). The most common and prominent spinal deformity is scoliosis16). Various neurologic problems associated with cervical dysraphism, diastematomyelia, and Chiari malformations, were also reported14). While the KFS patients may spend childhood period without any obvious symptoms, neck pain, radicular pain, or sometimes myelopathic symptoms can occur with age7). Other reported anomalies frequently associated with KFS are scoliosis (60%), renal anomalies (35%), deafness (30%), congenital heart disease (14%), cranial and facial asymmetry (13%), and cleft palate (10%)15). As an extraspinal anomaly, an aortic aneurysm was noted in the first case while no specific extraspinal anomaly was detected in the second case.
The symptoms experienced by patients with KFS depend on the severity of deformity. In patients with minimal involvement, anomalies are often incidental findings on radiological examinations, and most of them will lead a normal life without any obvious restriction in daily activities3). However, at least 35-40% of adult patients will experience 1 or more symptoms related with cervical spine, neck pain, radiculopathy, and myelopathy8). In both cases presented here, in addition to multiple cervical fusions, anterior translation of C1 has occurred secondary to kyphotic deformity of the fused upper cervical vertebrae, and was associated with symptoms of quadriparesis and decreased proprioception from spinal cord compression caused by the C1 posterior arch. In approximately 25% of KFS patients, spinal canal stenosis occurs due to congenital deformity or degeneration above, below, or at the level of fusion with cord compression5). Degenerative disorders including bulging disc, bony spur, ligament hypertrophy, stenosis, and instability, usually occur at the mobile segment adjacent to the fused vertebrae13). In the two cases of our study, cord compression occurred at the stenotic canal between kyphotic apex and C1 posterior arch caused by congenital deformity of cervical spine rather than degenerative stenosis.
Feil classified the syndrome into 3 types, based on the degree of cervical deformity, and the presence of deformities in other spinal regions; type I, massive fusion of the cervical spine; type II, fusion of one or two vertebrae; and type III, presence of thoracic and lumbar spine anomalies with either type I or II4). More recently, Samartzis et al. proposed another classification according to radiographic presentations limited to the cervical spine; type I, a single fused segment; type II, multiple noncontiguous fused segments; and type III, multiple contiguous fused segments17). Samartzis et al. reported that type I often had neck pain, whereas type II and III showed a higher incidence of developing radiculopathy or myelopathy5). Both of our cases were Samartzis type III and had radiculopathy and/or myelopathy, which conditions were consistent with the proposed clinical risk according to the Samartzis' classification.
The management of KFS is predominantly conservative. Samartzis et al. indicated that surgery is recommended if myelopathy or radiculopathy is refractory to conservative management5). In the majority of reported cases, myelopathy was related with spinal instability requiring surgical decompression with craniocervical fixation1,5,8). Atlantoaxial instability can be diagnosed on the basis of an ADI exceeding 4mm11), or a difference in neck flexion and extension exceeding 3.5mm6). Our cases do not seem to have C1-2 instability according to these criteria. However, according to the pervious papers, craniocervical fixation seemed to be undergone regardless of the presence of C1-2 instability1,5,8). KFS patients have a severe limitation of cervical motion due to multi-level fusion from C2 to lower cervical vertebrae, and the occiput-C1-2 levels remain as important motion preserved joints in cervical spine. Craniocervical fixation may deprive KFS patients with functional occiput-C1-2 joints of cervical motion near completely, which is the reason we should try to avoid craniocervical fixation if possible. Even though our cases were indicated for surgical decompression due to stenosis and myelopathy, spinal fixation was avoided because they showed stable C1-2 segment. For 2 years of follow up, there was no newly developed neurologic disorder or spinal instability.
In spite of the favorable outcome for 2 years after simple decompression without fixation, it seems to need longer follow up period and more number of cases to get more meaningful clinical evidence to confirm the ineffectiveness of craniocervical fixation in the KFS patients without spinal instability.
CONCLUSION
Patients with KFS are at risk of developing myelopathy due to stenosis between kyphotic apex and C1 posterior arch, which may be aggravated by excessive neck motion or posture. Early diagnosis of KFS will be helpful to prevent neurological problems in the patients. When surgical treatment is indicated, it seems simple decompression of C1 posterior arch without fixation is effective for not only resolving cord compression but also preserving occiput-C1-2 joints motion in the patients without C1-2 instability.