INTRODUCTION
The Chiari I malformation is an infrequently detected congenital anomaly characterized by the downward displacement of the cerebellum with a tonsillar herniation below the fora men magnum that may be accompanied by syringomyelia, hydrocephalus and increased intracranial pressure (IICP)6,14). Patient may be asymptomatic or may have a variety of neurologic symptoms, including headache, neck pain, visual disturbance, vertigo, and ataxia1). The most common presenting symptoms is headache. Surgery, such as foramen magnum decompression, is indicated for a symptomatic Chiari I malformation and Chiari I malformation with a syrinx, but incidental lesions may be followed-up without further treatment7).
There is no effective alternative to operative decompression for patients with a symptomatic Chiari I malformation12). However, the surgery is not always easy and may have complications, and patients should therefore be selected very carefully. Almost all of the patients who have a Chiari I malformation with a headache and a syrinx are offered surgical intervention to prevent permanent cord damage12). In addition, patients without a syrinx are offered surgical intervention when a refractory headache appears or objective neurological abnormalities exist4,12,16).
Headache is associated sometimes with IICP. However, IICP is associated with various causes, and the Chiari malformation may be an incidental finding.
We introduce a case of a Chiari malformation without a syrinx or hydrocephalus but with IICP that was caused by hyperthyroidism rather than by the Chiari malformation. The headache resolved after medical treatment for hyperthyroidism.
CASE REPORT
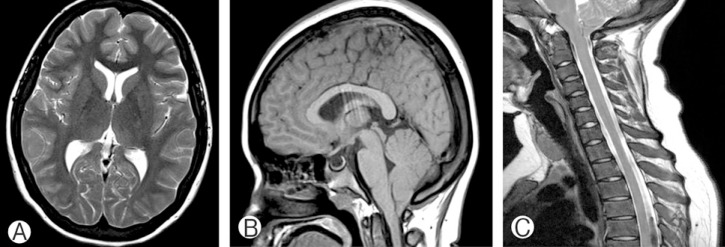
A nineteen-year-old girl visited our outpatient clinic complaining of a headache. The headache had started 3 months previously, followed by vomiting, and she could not concent rate on studying. A tingling sensation in the four extremities existed at the same time. She had lost 10 kg of her body weight during the 3 months (height 157 cm, weight 73 kg → 63 kg). Brain magnetic resonance imaging (MRI) showed a normal-sized ventricle, but cerebellar tonsillar herniation greater than 5mm, exactly 11mm from foramen of magnum was detected that was consistent with a Chiari I malformation (Fig. 1). The syringomyelia was not accompanied by a whole spine MRI. The Chiari I malformation was suspected as the cause of the IICP.
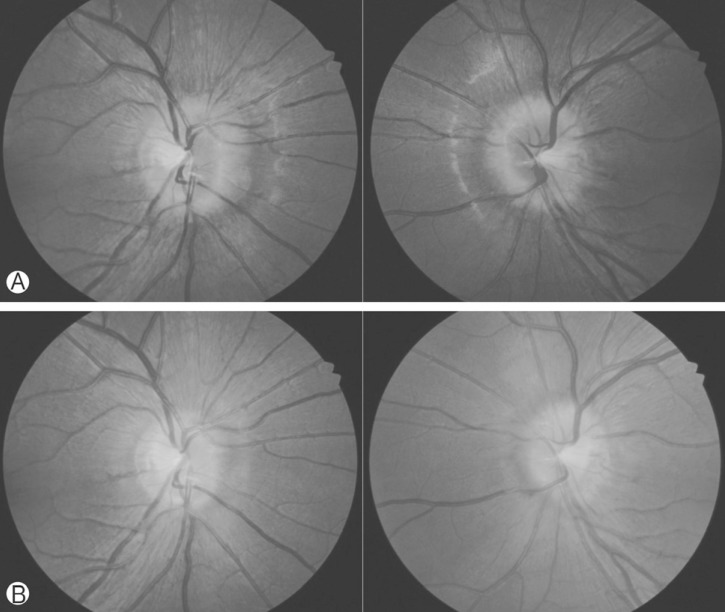
A papilledema was detected on both eyes on a fundus examination (Fig. 2A), and severe disc swelling with peripapillary retinal nerve fiber layer swelling was observed.
While considering foramen magnum decompression for a Chiari I malformation with IICP symptoms, she was referred to our institute. Then, an enlarged thyroid gland was detected on a physical examination, and a thyroid function test was conducted. The initial thyroid function test showed an elevated free T4 level (4.44 ng/dL, reference: 0.7-1.80 ng/dL), an elevated thyroid stimulating hormone (TSH) receptor antibody level (2.3 IU/L, reference: 0-1.1 IU/L) and a decreased TSH level (0.1 µIU/mL, reference: 0.25-4.00 µIU/mL). A thyroid ultrasonogram showed the diffuse enlargement of the thyroid with no hot or cold lesions, and the 99m-Tc scan's 20-minute uptake was 14.5%. All of these laboratory results confirmed the diagnosis of hyperthyroidism, and the presence of the TSH receptor antibodies confirmed Graves' disease.
Therefore, the patient underwent medical management with methimazole (10-5mg) and 40mg of propranolol (a beta adrenergic antagonist). After 2 weeks of medical management, she did not complain of headaches (Table 1). A fundus examination 3 weeks later showed that the fundus had returned to normal on both eyes (Fig. 2B). Her headache did not return during 6 months of follow-up. Consequently, she did not undergo a foramen magnum decompression.
DISCUSSION
The Chiari I malformation consists of the caudal displacement of the cerebellar tonsils into the upper cervical spinal canal, and it is commonly associated with syringomyelia or hydrocephalus. The most common symptom is headache, and other common symptoms include weakness or numbness, loss of temperature sensation, and unsteadiness8).
Cerebrospinal fluid (CSF) flow studies using cine phase contrast MRI have demonstrated that many children with symptomatic Chiari I malformations have an abnormal CSF flow at the foramen magnum9). Many clinical series advocate a posterior fossa craniectomy, including a suboccipital craniectomy and the removal of the C1 posterior arch, for the decompression of the cerebellum and the cerebellomedullary junction, along with an augmentative duroplasty for treating symptomatic patients with Chiari I malformations. There is a general consensus that the incidental discovery of asymptomatic patients with Chiari I malformations ordinarily does not make them candidates for surgical intervention13).
There have been rare cases of hyperthyroidism with increased intracranial pressure; moreover, there has been no case of hyperthyroidism with a Chiari malformation. Coutinho et al.2) showed a case of 31-year-old woman with clinical symptoms and laboratory confirmation of Graves' disease that presented as pseudotumor cerebri. Stern et al.15) showed a case of 29-year old woman who had headache and laboratory confirmation of Graves' disease with occult hydrocephalus that became symptomatic during episode of thyrotoxicosis. Herwig et al.5) showed a case of 32-year-old woman presenting with progressive symptoms of IICP and slight enlargement of the ventricle on CT scan. The underlying case was hyperthyroidism due to Graves' disease.
In hyperthyroidism, an increased cerebral blood flow with increased cerebral blood volume can cause IICP. IICP is associated with an elevated cerebral blood volume, with osmotic or vasogenic cerebral edema from the increased CSF outflow resistance at the arachnoid villi and with high cerebral venous pressure10). Hyperthyroidism has been shown to increase the cerebral blood flow, which has been correlated with increased cerebral volume, and consequently IICP3,11). There is also the theory that due to the increased general metabolic turnover associated with thyroid hormones, the CSF turnover and production is increased5). However, whether the detailed mechanism of IICP in hyperthyroidism is due to the altered intracerebral hemodynamics with a secondary rise in the ICP is debated.
Headache, nausea, vomiting, and papilledema present as the primary features of IICP16). In the present case report, the patient complained of headache, which was caused by IICP, and the IICP was caused by Graves' disease or the Chiari I malformation.
Medical treatment for hyperthyroidism was started preferentially, and the presenting symptom abated without further surgical intervention for the Chiari I malformation.