INTRODUCTION
A large increase in fusion rates for spine surgery has been observed in the last 20 years9), and the frequency of revision spine surgery continues to increase. The most common reasons for additional surgery7) following fusion surgery are implant complications and pseudoarthrosis.
It is necessary to remove and change the existing implants during revision surgery. The keyholes inside each screw brand (particularly polyaxial screws) are different. They may be in the shape of a male or female rectangle or hexagonal, octagonal, or star-shaped. Therefore, it is necessary to have the instrument set used during the first operation or to have an appropriate screwdriver available. This is not always possible and in some circumstances the implant may no longer be in production.
When revision surgery studies were examined5,12), methods to remove broken screws are reported but very little information related to removing normal screws has been provided. No previous report has described a single-piece screw remover to remove normal screws. A small part of the rod is cut and placed in the screw when a removal set is not available. After tightening the screw head, mobile screw's head become monoblock screws. This screw is a single piece that can be removed by hand or with pincers10). The polyaxial remover presented here requires only a cap-screw screwdriver to remove the polyaxial screws. Due to the structure of the remover and the method, existing screws can be removed with minimal dissection of surrounding soft tissue.
Surgical techniques for revising the spine take longer than those of primary spine surgery. Debridement is important to remove scars, envision the bone elements, and prepare a new fusion bed during revision surgery. Extended operating time increases blood loss and infection risk8). Additional procedures applied to remove screws cause the surgeon to expend extra effort, which may lead to loss of time. Our tool simplifies and accelerates the screw removal process; thus, shortening operating time. There is also a need for large metal cutters to cut rods. The aim of our polyaxial screw remover design is to facilitate screw removal and thereby reduce blood loss, infection risk, cost, and effort expended by the surgeon.
MATERIALS AND METHODS
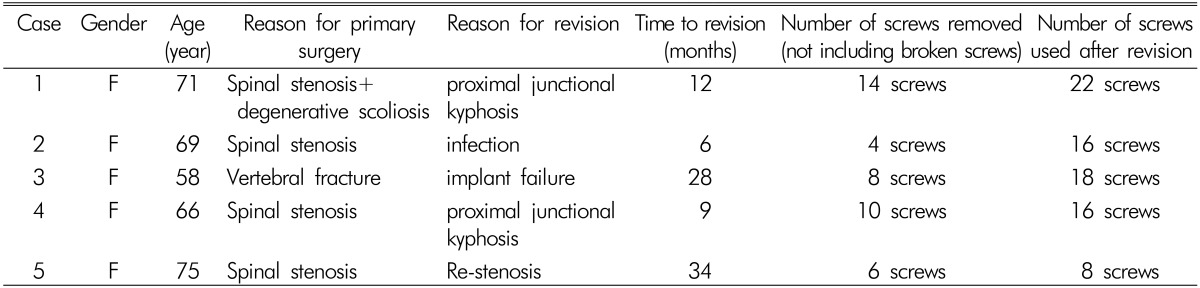
The patient demographic data and reasons for primary and revision surgery are given in Table 1. The aim when removing polyaxial screws is to stabilize the polyaxial head so the screw becomes monoaxial and can be removed by turning. The method described by Kose et al.6) was of benefit when we designed our instrument, which has not been described previously in the literature. In the method of Kose et al., the screw becomes monoaxial with a rod and cap screw, whereas we used a U-shaped end section in our instrument without the need for a rod.
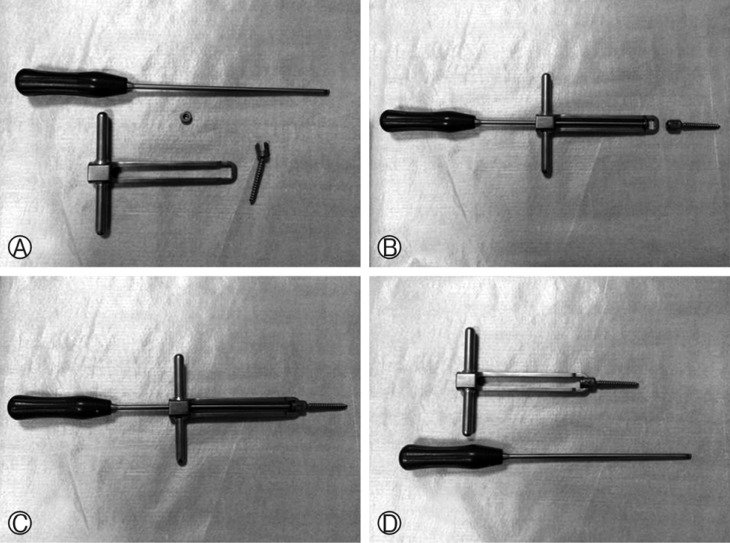
The polyaxial remover consists of a single-piece shaft, sleeve, and handle (Fig. 1A, B). The shaft section is hollow, and the screw cap is tightened with a screwdriver. The U-shaped end section has a narrower structure (Fig. 1B). Thus, a spine screw enters easily, and the surgeon avoids damaging surrounding tissue.
The head section of a polyaxial screw was removed, and the screw was placed in the U-section (Fig. 2). The cap screw was tightened on the screw, and the screw was fixed in the end section of the apparatus. The polyaxial screw that became monoaxial can be removed by turning the handles on the shaft. Thus, the need for metal cutters and extra time and effort is avoided. This method also removes the need to clean the fibrous tissue covering the internal screws and to see the screw shape.
RESULTS
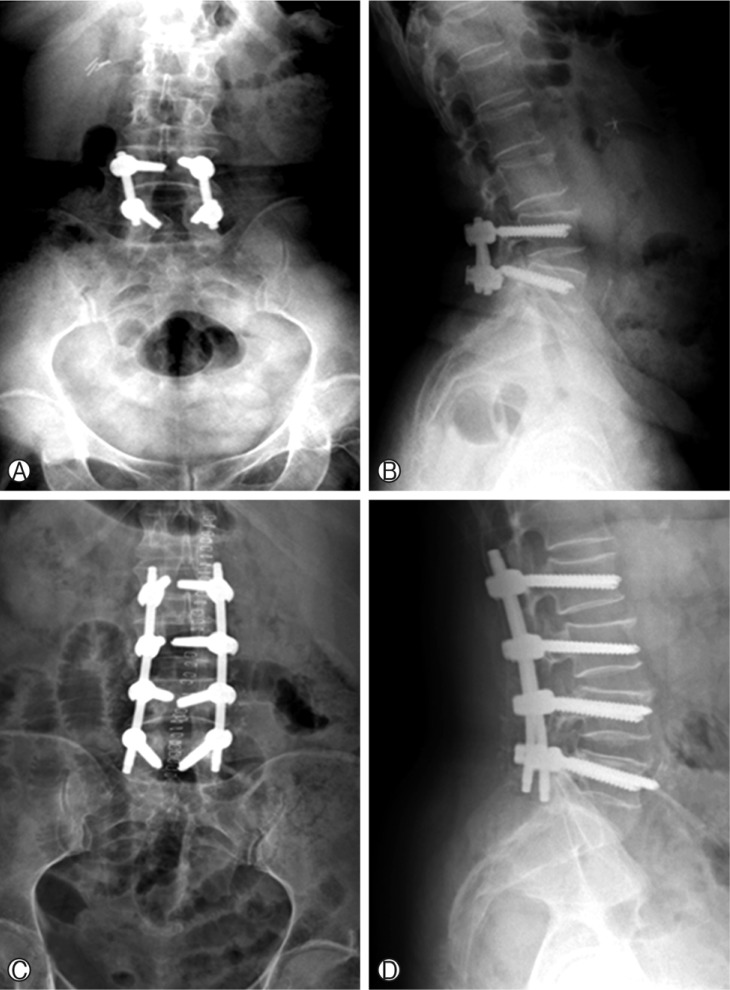
A total of 42 polyaxial screws were removed from five patients with the new single-piece screw remover (Fig. 2) (Table 1). The pedicle and surrounding soft tissue were not damaged during screw removal. The polyaxial cap screws were 4.5 hexagonal screws in four patients and star-shaped in one patient. After removing the cap screws and rods, all of the polyaxial screws were made monoaxial with the instrument described above and were removed rapidly in a minimally invasive way with no complications. No neurogenic changes developed during surgery.
DISCUSSION
We have described a screw removal instrument designed to overcome the problems of screw removal often encountered during revision surgery. Our clinical application shows that these screws can be removed without the need for additional materials or soft tissue debridement within or below the screw head.
The correct screwdriver for the materials used cannot always be obtained to remove existing implants during revision surgery because of the different designs. Therefore, additional techniques and materials are required. This explains why revision surgery can be a longer and more fatiguing operation with increased blood loss.
Of the several known spine surgery problems, the most accepted and most widely used method for repair is pedicle screw fixation1,2,3,4,5,6,7,8,9,10,11). After fixation, the most common reasons for revision surgery7) are implant problems and pseudoarthrosis. Implant failure3,4) has been reported at rates of 3-12%. Methods and instruments to remove broken screws have been described in the literature5,12). However, no additional methods6,10), other than the rod techniques for removing normal screws, have been described. In the U-rod technique described by Köse et al.6), the cap screws are removed with an Allen key, and the screw is placed in the U-shaped rod after removing the rods. After tightening the screw head, the screw with a mobile head becomes a monoblock screw. This single-structure screw can be removed by hand or with pincers. All of these procedures result in extra effort, leading to loss of time. Cutting rods in good condition is a loss of material. In addition, large metal cutters are required to cut the rods, a rod bender is needed to shape, and pincers are needed to turn the rod placed on the screw head. Our screw remover design is a single piece and will not damage surrounding tissue or the pedicle (Fig. 1A, B). There is no need for metal cutters or a rod bender; thus, reducing the time and effort required. The tool also removes the need to clean the fibrous tissue covering the internal screws to determine screw shape. Thus, bleeding associated with debridement of fibrous tissue is prevented.
There were several limitations to this study. First, the number of patients was relatively small. Second, a polyaxial remover was used after removing the cap screws, so it was necessary to have a screwdriver suitable for the cap screws. However, cap screws are generally hexagonal or star-shaped and there are few varieties. These screws are generally found in sets, or the screwdriver in the revision set can be used. Another limitation was that the polyaxial remover could not be used if the cap screw is damaged or broken.
The screw removal technique using the polyaxial remover is practical and easy and requires a minimal amount of time. As presented here, 42 screws were removed from five patients without any complications. A polyaxial remover or a similar instrument has not been reported previously. This newly designed polyaxial remover is recommended for use in all revision vertebral surgeries.