INTRODUCTION
Spinal arachnoid cysts are a rare cause of spinal cord compression. These cysts most commonly occur in the middle to lower thoracic spine but also have been reported in the lumbar, lumbosacral, and thoracolumbar regions5,6,7,10). Extra-dural arachnoid cysts develop from protrusions of arachnoid herniating through a small dural defect, and cyst enlargement can result in symptomatic spinal cord compression5). The presenting symptoms may include pain, paresthesia, neurogenic intermittent claudication, bowel or bladder dysfunction, and variable degrees of spastic weakness. The cysts have a pedicle in communication with the spinal subarachnoid space and, because of their origin, contain CSF9). MRI is the diagnostic procedure of choice as it is noninvasive and can demonstrate the nature of cyst, size, and the anatomic relationship with the spinal cord.
The etiology and pathogenesis of spinal extradural arachnoid cysts are not clear. Although they most probably have a congenital origin, some may be acquired from trauma, iatrogenic damage, hemorrhage, meningeal infection, or inflammation3,5,13). Spinal extradural arachnoid cysts are usually considered to present outpouching of the arachnoid through a small dural defect to form an arachnoid hernia or arachnoid diverticula11). In this article, we report a case of spinal extradural arachnoid cyst of probable traumatic origin treated with surgical obliteration of the communicating dural defect.
CASE REPORT
1. Presentation and Examination
A 65-year-old male patient with history of fall-down injury from a cliff 50 years ago presented progressive paraparesis from 15 years following trauma. At the time of injury, the patient had transient back pain and returned to his normal daily life as a laborer after recovering from lumbago. After 15 years from the accident, mild motor weakness of bilateral legs developed, which progressed slowly, and the patient had been unable to walk since 35 years from the time of injury. Voiding difficulty and urinary incontinence developed two years ago. On admission, the patient presented motor power of grade two at both lower extremities, and ambulation was impaired. Muscle atrophy of both lower extremities was prominent. Knee jerk and ankle jerk were absent bilaterally. The patient had no significant underlying diseases.
2. Imaging Findings
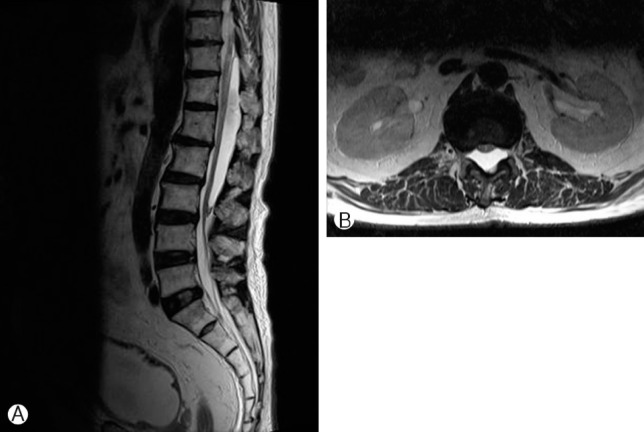
Whole spine MRI revealed long segmental cystic lesion of CSF signal intensity at dorsal extramedullary space of T11 to L3 level suggesting arachnoid cyst with diffuse cord compression (Fig. 1A, B). The spinal cord was displaced anteriorly and flattened. Associated findings included nerve root sleeve cyst at T2 to T3 level located leftwardly. Electromyelography revealed bilateral lumbosacral polyradiculopathy consistent with cauda equina syndrome of chronic state.
3. Operation
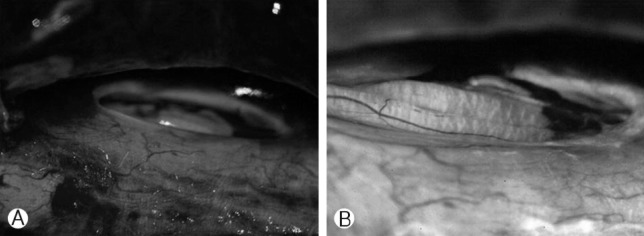
The arachnoid cyst was exposed by total laminectomy of T12 and extended laminotomy to L1 level. Large sized epidural arachnoid cyst was located dorsal to the dural tube. On exposure, 7×5 mm sized ovoid shaped dural defect was identified at right sided dorsolateral aspect of the dura mater between nerve root sleeves at T11 and T12 level (Fig. 2A, B). The cyst contained clear fluid suggestive of CSF. Microsurgical repair of the dural defect was performed using two sutures and application of collagen fleece (Tachocomb®) and fibrin glue (Tissucol®). Following repair of the dural defect, no further leakage of CSF was verified on Valsalva maneuver in head-up position.
4. Postoperative Course
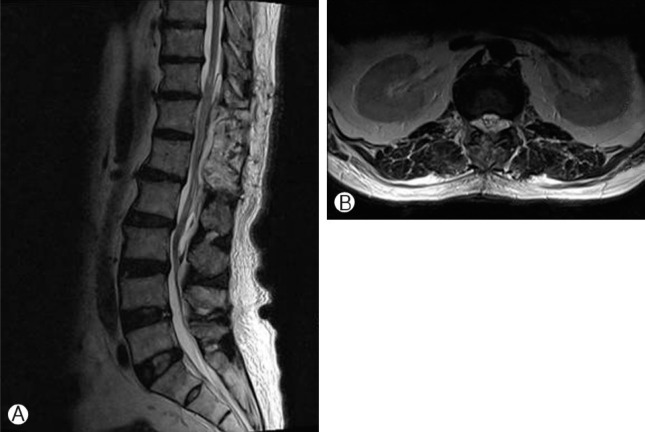
Histologic examination of the cyst wall revealed pathological diagnosis as arachnoid cyst. Postoperative MRI evaluation performed at 1 month following the surgery revealed decreased size of arachnoid cyst at T11 to L3 level along with decompression of the flattened spinal cord (Fig. 3A, B). The neurological status including motor power of both lower extremities was stationary on follow-up examination at 5 months postoperatively. The patient is currently on supportive rehabilitation therapy.
DISCUSSION
Extradural arachnoid cysts of the spine are an uncommon cause of myelopathy secondary to spinal cord compression6,8,11). The exact mechanism of the formation of spinal arachnoid cysts is not yet identified. In the adult population, several theories have been postulated. These can be divided into five categories as congenital; arachnoid adhesions secondary to an inflammatory process caused by virus, spirochetes, or bacteria; arachnoiditis secondary to subarachnoid hemorrhage, contrast media, spinal anesthetics, meningitis; traumatic injuries to the vertebral column, lumbar punctures used in diagnostic procedures, or anesthetic and intradural surgery; and idiopathic10,12,14). It was previously documented that congenital asymptomatic cysts could be enlarged due to trauma and become symptomatic8,11). Pulsatile CSF dynamics, osmotic gradient between the subarachnoid space and cyst, and the valve-like mechanism between the cyst and subarachnoid space may play an important role in the enlargement of spinal extradural arachnoid cysts5).
Most cases of spinal arachnoid cysts are idiopathic, and those of traumatic origin are especially rare. In all cases, however the disease results from the herniation of the arachnoid through a defective or fragile dura mater5,12,13). In cases of spinal arachnoid cysts of congenital origin, most patients are presented in adolescence or in early adult life, and the diverticulum tends to be located at central regions, but intraoperative findings in this patient showed lesion at dorsolateral aspect of the dura3,9). In this case, there was a definite spine injury, and we postulate that the cyst was of traumatic origin, caused by herniation of the arachnoid membrane through a traumatic defect in the inner layer of the dura mater. Probably a tiny tear was made at right-sided dorsolateral aspect of the lower thoracic dura when the patient was injured, and intact arachnoid bulged out through the opening later on. We presume that because of the one-way valve effect leading to entrapped CSF collection of passive dynamics, the cyst grew larger, eventually compressing the spinal cord. The arachnoid out-bulging enlarged gradually to form an epidural arachnoid cyst. The epidural arachnoid cyst became large enough to compress the conus medullaris and cauda equina, causing paraparesis about 20 years after the fall-down injury.
During the surgery, no definite laminar signs indicating sustained compression fracture or injury of the posterior elements were observed. Stretching and partial avulsion of the nerve root structures may have caused arachnoid and dural tearing during the time of trauma, causing subsequent collection of CSF at the epidural space, communicating freely between subarachnoid space and dural sleeves of the roots.
Surgical treatment is required when neurological symptoms develop due to cyst induced spinal cord or nerve root compression1,2,11). Although numerous surgical treatment methods have been proposed, the results of surgery were variable. Preoperative myelomalacia and long duration of symptoms have been implicated as being predictive of poor surgical outcome. The operative treatment most commonly advocated has been total excision of the cyst2,5,13). However, removal may be hazardous and entail the sacrifice of nerve roots with risk of diverse complications including adherence of the cyst to the nerve roots or to the spinal cord.
CONCLUSION
The etiology, pathogenesis and treatment of the spinal extradural arachnoid cysts have not been well established. In surgery, dural defect should be repaired. Neurological recovery seems to depend on the size of the cyst and the degree and duration of the spinal cord compression. Long-standing myelopathy is unlikely to show significant improvement, as observed in the current case report. Therefore, in delayed cases, surgery may be offered as an intervention with prophylactic purpose to prevent further neurological impairment, rather than a curative management. Surgical treatment of spinal extradural arachnoid cysts could provide neural decompression and prevent cyst refilling.
Neglecting the neurological symptoms for about 35 years had regretfully resulted in dense, almost irreversible paraparesis and neurogenic bladder. Such a delayed-onset spinal extradural arachnoid cyst should be taken into consideration on the differential diagnosis of intraspinal cysts.