INTRODUCTION
Cervical total disc replacement (TDR) has been one of the most commonly performed procedures for the treatment of cervical radiculopathy since Dr. Goffin implanted Bryan (Medtronic Sofamor Danek, Memphis, TN, USA) artificial disc for the first time in January 2000. And it has been thought as an alternative method to traditional anterior cervical discectomy and fusion (ACDF).
TDR has some advantages compared with ACDF1,8). It maintains physiologic range of cervical motion and the mechanical characteristics of functional spinal unit. TDR especially has been known to prevent or decrease the risk of adjacent segment degeneration.
There are, however, several complications in cervical TDR including postoperative kyphotic deformity.
Some causes have been suspected to lead to postopera tivekyphotic deformity. Yoon et al.14) suggested over-milling at the dorsal endplate, artificial disc insertion angle, structural absence of lordosis in Bryan artificial discprosthesis, removal of posterior longitudinal ligament, pre-existing kyphosis. Yi et al.13) proposed the correlation between insertion depth of the Bryan artificial disc prosthesis and postoperative kyphotic deformity.
The purpose of this study is to investigate the correlation between insertion depth of Prodisc-C(Synthes Inc., West Chester, PA, USA) artificial disc and postoperative kyphotic deformity after TDR surgery, and the range of artificial disc insertion depth to prevent postoperative whole cervical or segmental kyphotic deformity.
MATERIALS AND METHODS
A retrospective analysis of medical record and radiogra phsof 50 patients was performed. They admitted to Korea University Anam Hospital, Seoul, Korea, and underwent on a single-level cervical TDR surgery with Prodisc-C artificial disc between July 2004 and June 2011.
Before the surgery, all patients were evaluated using cervical X-ray and magnetic resonance imaging. C2-7 Cobb's angles, segmental angles of the operative level with static neutral lateral X-ray were measured to evaluate pre- and post-operative final cervical sagittal balance and to investigate the postoperative kyphotic deformity.
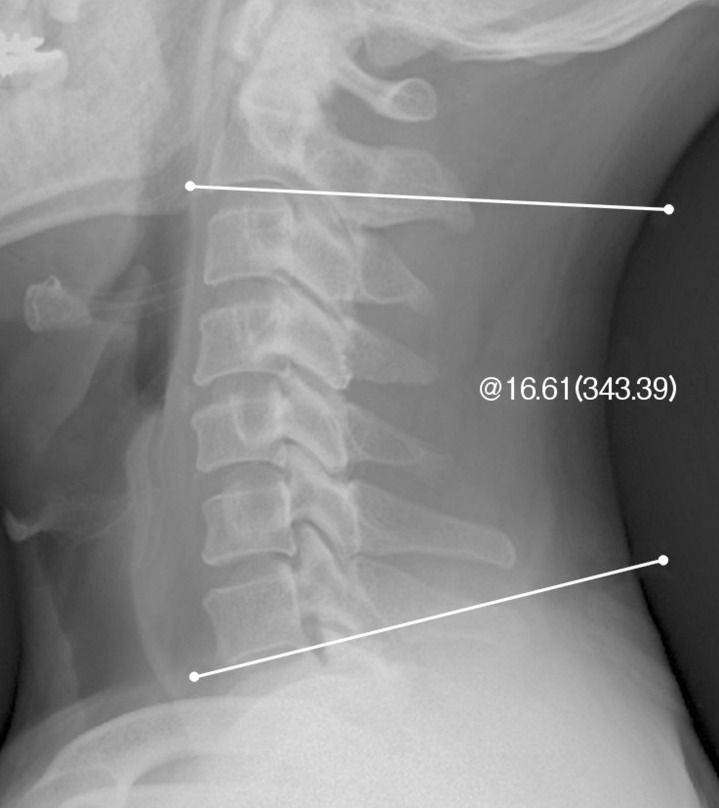
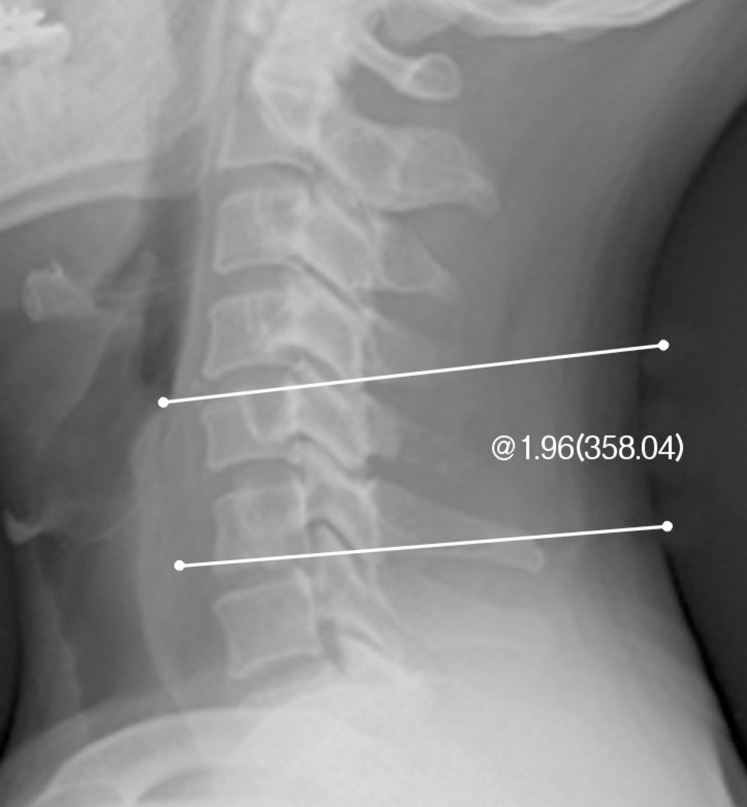
C2-7 Cobb's angles were measured with the standard Cobb's angle method between the inferior margin of C2 and C7 vertebral bodies in a neutral position (Fig. 1). Segmental angles of the operative level were measured between the superior margin of upper cervical vertebral body and the inferior margin of lower cervical vertebral body (Fig. 2). A negative value means lordosis of cervical spine and a positive value means kyphosis.
Insertion depth of Prodisc-C artificial disc was calculated by a formula suggested by Yi et al.13) as shown below. The length from the line connecting the posterior corner of superior and inferior vertebral bodies to the line connecting anterior corner of superior and inferior vertebral bodies at the operated disc level was measured. Then the length from the posterior body line to the center of the Prodisc-C artificial disc on the lateral cervical X-ray was measured (Fig. 3). But in this study, a modification was applied to the formula. 50% subtraction was not performed to estimate the insertion depth of Prodisc-C artificial disc from posterior vertebral margin. An insertion depth value of Prodisc-C artificial disc larger than 50% indicates that the disc location is anterior to the center of vertebral body and a smaller value than 50% indicates the location is posterior to the center of vertebral body.

There are many different reports to define normal cervical lordosis and postoperative kyphotic deformity. With each of the definitions, we tried to find out any statistically significant correlation between artificial disc insertion depth and postoperative kyphotic deformity.
At first, we introduced the definitions that Heary and Karimi4) proposed. Postoperative kyphotic deformity was defined as a loss of the normal lordotic cervical curvature of at least 5 degrees per motion segment (C2-7). With reference to this definition, the patients were divided into 2 groups as those with postoperative kyphotic deformity or not. And their insertion depths of Prodisc-C artificial disc were analyzedstatistically to find difference of mean value.
Then we used the definition that Gore et al.3) proposed as normal cervical lordosis. In men, C2-7 Cobb's angle more than 22° was defined as 'hyperlordotic', C2-7 Cobb's angle less than 16° was defined as 'kyphotic' and that between 16° and 22° was defined as 'lordotic'. And in women, normal C2-7 Cobb's angle was from 15° to 25°, C2-7 Cobb's angle more than 25° was defined as 'hyperlordotic', and C2-7 Cobb's angle less than 15° was defined as 'kyphotic'. When a patient's postoperative C2-7 Cobb's angle changed from 'hyperlordotic' to 'lordotic', 'hyperlordotic' to 'kyphotic' or 'lordotic' to 'kyphotic', we hypothesized that the patient showed postoperative kyphotic deformity. We analyzed those with postoperative kyphotic deformity to find out any difference from others.
But the methods using the definitions that Gore et al.3) pro posed can't distinguish those whose postoperative C2-7 Cobb's angle changes within the ranges of normal lordotic curve. So other concept of postoperative kyphotic deformity was introduced. When a patient'spostoperative C2-7 Cobb's angle decreased more than 5% of preoperative C2-7 Cobb's angle, he/she was hypothesized to show postoperative kyphotic deformity and analyzed to search any correlation with artificial disc insertion depth.
Finally, pre- and post-operative segmental angles were evaluated. When a patient's postoperative segmental angle of operative level decreased more than 5% of preoperative one, we hypothesized that the patient showed postoperative kyphotic deformity. On the contrary, when postoperative segmental angle of operative level increased more than 5%, we assumed that the patient showed postoperative lordotic change. When the range of changes was within 5% of preoperative segmental angle of operative level, we hypothesized that the patient didn't show any deformity. These 3 groups were analyzed statistically with insertion depths of Prodisc-C artificial disc using ANOVA test.
Pre- and post-operative C2-7 Cobb's angles and segmental angles of operative level were measured with quantitative measurement analysis software, PACS workstation (Centricity 2.0; General Electric Medical Systems, Milwau- kee, WI, USA). This program uses extrapolative algorithms to calculate the intersecting angle between 2 lines drawn by the investigator.
1. Statistical analysis
Statistical analysis was performed to search the correlation between insertion depth of Prodisc-C artificial disc and postoperative kyphotic deformity, and to estimate insertion depth of Prodisc-C artificial disc to prevent postoperative kyphotic deformity. Analysis of variance (ANOVA) test with SPSS software for Windows (version 20.0; SPSS Inc., Chicago, IL, USA) was performed.
RESULTS
Patients consisted of 31 men and 19 women, a ratio of 1.63: 1. Mean age was 48.84 years (range, 26-77 years). The mean duration of follow-up was 19.2 months (range, 9-28 months). Preoperative diagnosis included cervical herniated nucleus pulposus (41 patients), cervical spondylosis (8 patients), and foraminal stenosis (1 patient). The operated levels are as the following: C3/4 (3 patients), C4/5 (7 patients), C5/6 (29 patients), C6/7 (11 patients) (Table 1).
Mean disc insertion depth was 53.98%, ranging from 42.41 to 67.63%. An insertion depth value of Prodisc-C artificial disc larger than 50% indicates that the disc location is anterior to the center of vertebral body, and a smaller value than 50% indicates the location is posterior to the center of vertebral body, as mentioned above.
According to the definition that Heary and Karimi4) proposed, fifteen patients were classified at the group with postoperative kyphotic deformity. And their mean disc insertion depth was 53.33%. But the mean disc insertion depth of the rest thirty-five patients was 54.26%. So the result of analysis didn't show any difference between the group with postoperative kyphotic deformity and the other group without postoperative kyphotic deformity (Table 2).
Gore et al.3) proposed that a 16° to 22° cervical lordosis in men and a 15° to 25° cervical lordosis in women were normal. According to this definition, the patients were divided into three groups including 'hyperlordotic', 'lordotic' and 'kyphotic'. And we analyzed those who were hypothesized as postoperative kyphotic deformity to search any correlation with insertion depths of Prodisc-C artificial disc. But the group with postoperative kyphotic deformity didn't show any statistical significant difference in insertion depths of Prodisc-C artificial disc from other groups (Table 2).
According to the concept that decrease more than 5% in postoperative C2-7 Cobb's angle is assumed as postoperative kyphotic deformity, twenty-six patients were classified as the group with postoperative kyphotic deformity. We analyzed them statistically to search any correlation with artificial disc insertion depth. But no significant difference was found from the others, either (Table 2).
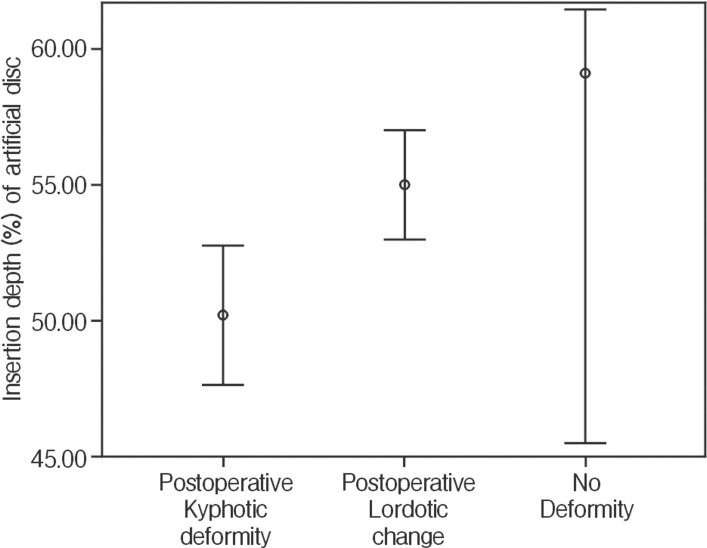
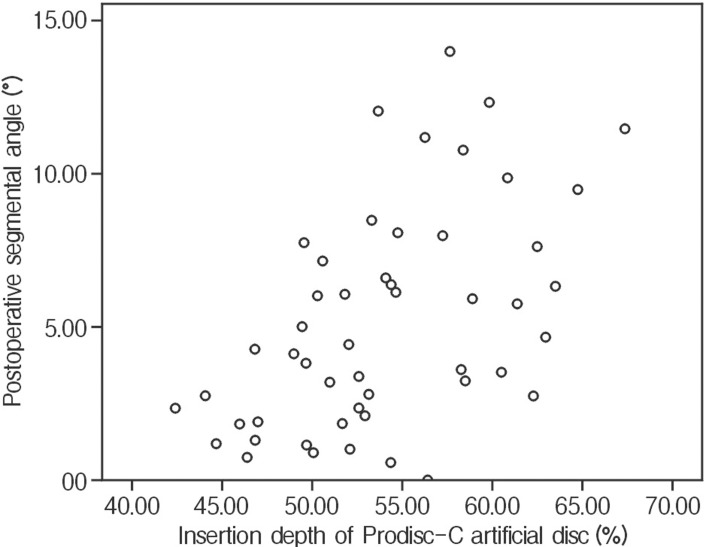
Finally, the patients were classified into three groups according to the changes between preoperative and postoperative segmental angles. Mean artificial disc insertion depth of those who showed postoperative kyphotic deformity in segmental angle was 50.18±4.23%. And mean artificial disc insertion depth of those with postoperative lordotic change and those without postoperative deformity were 54.98±5.76% and 59.10±5.49%, respectively. Mean artificial disc insertion depth of the group with postoperative kyphotic deformity was smaller than that of the group with postoperative lordotic change or the group without postoperative deformity (p<0.05,Fig. 4). Positive correlation was found between artificial disc insertion depth and postoperative segmental angle (R=0.516, p<0.001,Fig. 5). These two results mean anterior located disc led to lordotic postoperative segmental angle and posterior located disc led to kyphotic segmental angle.
But the range of artificial disc insertion depth in the group with postoperative kyphotic deformity in segmental angle was not apart from that of the group with postoperative lordotic change (Fig. 4). The confidence interval of the group with postoperative kyphotic deformity in segmental angle was from 47.63 to 52.75%, and that of the group with postoperative lordotic change was from 52.97 to 56.99%. Technically these two confidence intervals don't overlap. But it failed to estimate proper insertion depths of Prodisc-C artificial disc effective in preventing postoperative kyphotic deformity.
DISCUSSION
As an alternative surgery to ACDF, TDR surgery has been an emerging procedure for cervical radiculopathy. Many authors have reported that TDR shows similar or better clinical outcomes8,10), or some advantages compared to ACDF1). However cervical TDR has several complications including postoperative kyphotic deformity. Xu et al.12) reported 60% of their patients developed endplate kyphosis. Johnson et al.5) found 80% of their single-level TDR patients with Bryan artificial disc developed endplate kyphosis.
Recently, several design limitations and contributing factors for postoperative kyphotic deformity were raised in the literature. Yoon et al.14) reported that postoperative kyphoticdeformity after TDR with Bryan artificial disc was caused by several factors, including over-milling at the dorsal endplate, the insertion angle of Bryan artificial disc, structural absence of lordosis in the Bryan artificial disc, surgical procedure to remove the entire posterior longitudinal ligament, and pre-existing kyphosis. Cao et al.2) reported over-milling or asymmetric milling of dorsal endplate influences on the disc insertion angle and leads to postoperative kyphotic deformity. Yi et al.13) reported that toprevent postoperative kyphotic deformity after TDR with Bryan artificial disc, intentional modificationin disc insertion angle and depth would be helpful.
But Prodisc-C artificial disc is more sensitive to the surgical location of device than Bryan artificial disc, because Prodisc-C artificial disc has fixed center of rotation (COR) but Bryan artificial disc has variable COR. So Prodisc-C artificial disc needs to be confirmed about the correlation between the insertion depth of artificial disc and postoperative kyphotic deformity.
This study was focused to investigate the correlation between insertion depth of Prodisc-C artificial disc and postoperative kyphotic deformity, and the range of artificial disc insertion depth effective in preventing postoperative kyphotic deformity.
Postoperative segmental angle of operated level showed positive correlation with insertion depth ofProdisc-C artificial disc, but postoperative C2-7 angle didn't show any correlation with insertion depth of Prodisc-C artificial disc.
The group with postoperative segmental kyphosis had smaller insertion depth of Prodisc-C artificial disc compared to others. But when patients were classified into postoperative C2-7 kyphosis group according to several definitions of cervical kyphosis, none of them showed any statistical difference in insertion depth of Prodisc-C artificial disc. This result was similar to that of Yi et al.13) reported.
There are some literatures that postoperative kyphotic deformity isn't associated with clinical outcomes6). But once kyphosis has developed, axial loads tend to cause further kyphosis, thus initiating a vicious cycle and progression of the deformity. And cervical kyphosis tends to developan associated neurological deficit or chronic neck pain11). So postoperative kyphotic deformity is undesirable condition and should be avoided after TDR surgery.
There are some weaknesses in this study. First of all, other factors that may influence postoperative kyphotic deformity weren't controlled enough. For example, overmilling of dorsal endplate is one of the most important factors that can induce postoperative kyphotic deformity2,14). But as a rule, we keel the dorsal endplate before the insertion of Prodisc-C artificial disc, not mill. And the number of cases wasn't enough to subdivide according to the degrees of milling. So whether milling was performed or not and the degrees of milling weren't included as variables. This uncontrolled factor may lead to the unproven correlation of postoperative C2-7 kyphotic deformity and insertion depth of Prodisc-C artificial disc. And the definitions of normal cervical lordosis and postoperative kyphotic deformity need more research. Third, many patients have been lost in outpatient follow-up and the periods of evaluating postoperative kyphotic deformity are irregular. If postoperative kyphotic deformity proceeds in course of time after surgery, it needs to be controlled, too. Clinical outcomes after surgery weren't evaluated or analyzed according to the degree of postoperative kyphotic deformity.
CONCLUSION
Postoperative segmental kyphotic deformity was associated-with insertion depth of Prodisc-C artificial disc. Anterior located artificial disc leads to lordotic segmental angle and posterior located artificial disc leads to kyphotic segmental angle postoperatively. But C2-7 Cobb's angle is not affected by artificial disc location after surgery. Further study with compensating weak points is required.