INTRODUCTION
Vertebroplasty, a surgical procedure involving the injection of polymethyl methacrylate (PMMA) into a collapsed vertebral body6), was first described in 1987 by Pierre Galibert and Herv├® Deramond for the treatment of symptomatic or aggressive vertebral angioma15). This technique has received significant attention and several studies related to the treatment of vertebral osteoporotic fractures have been published4,5,12,15,19).
Pain relief and stabilization of collapsed vertebrae are the goals of this procedure. Several previous studies revealed that this goal was achieved immediately after treatment18). However, long-term effectiveness is still questioned2,9,10). Furthermore, there are controversies regarding the optimal volume and distribution of the injected cement, and the association between clinical improvement and radiological changes18).
The purpose of this study was to assess the clinical and radiological results, elucidate the association between these results, and investigate radiological changes according to the distribution pattern and amount of injected cement after vertebroplasty.
MATERIALS AND METHODS
1. Patients
From January 2005 through October 2010, we performed vertebroplasty in 201 patients. Inclusion criteria were osteoporotic fracture with 5-20% canal encroachment and bone mineral density less than -3.0. Exclusion criteria included combined neurological deficits, pathological fractures, and unstable vertebral fractures involving the middle or posterior column. In patients <80 years of age, we treated preoperatively with postural reduction for approximately 2 weeks; in patients >80 years of age, we performed vertebroplasty immediately after the onset. Fifteen of the 201 patients who underwent vertebroplasty were available for follow-up for more than 2 years and underwent follow-up radiography at 6, 12, and 24 months after the procedure. We reviewed the radiological and clinical data retrospectively.
2. Vertebroplasty technique
The patients were placed in a prone position. An 11 Gage vertebroplasty needle was inserted via a transpedicular approach by using Siremobil Iso-C3D(Siemens Medical Solutions, Erlangen, Germany). The needle was advanced through the pedicle, sloping anteriorly, medially, and caudally. The needle tip was placed at the anterior one-third of the vertebral body. Once the needle was placed inside the vertebral body, the liquid and powder components of PMMA were mixed and injected steadily at 1.5 cc per minute through the needle under fluoroscopic guidance. Cement injection was performed under continuous fluoroscopic monitoring on lateral view, with close attention to the posterior margin of the vertebral body and the epidural space. During PMMA injection, frequent fluoroscopic controls were required to ensure that the material remained within the vertebral body without migrating into the surrounding venous plexus. Injection was terminated when the vertebral body was adequately filled or when the cement reached the posterior quarter of the vertebral body. After vertebroplasty, the patients rested in a supine position for 3-4 hours.
3. Imaging assessment
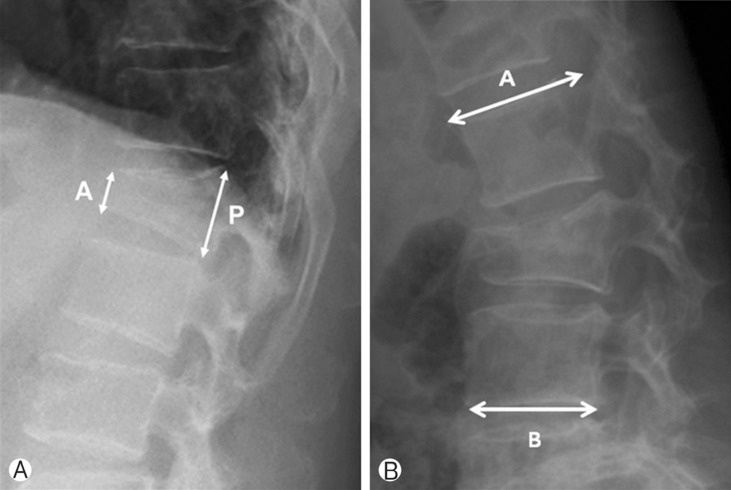
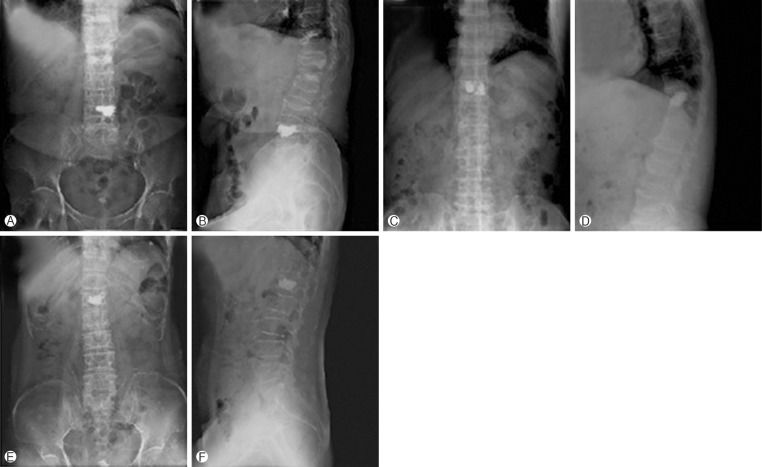
We measured preoperative and postoperative vertebral body compression ratios (so-called wedge deformity), by calculating the anterior-posterior (AP) ratio, the Beck23) Index (Fig. 1-A), and wedge angle (kyphotic angle), by measuring the angle between the superior endplate of the vertebral body above and the inferior endplate of the vertebral body below the fractured vertebra on the lateral radiograph1) (Fig. 1-B). For analysis of the injected cement pattern, we grouped the patients according to cement distribution as follows: group 1, unilateral, unilateral distribution of cement; group 2, bilateral-uneven, bilateral distribution of cement but separated mass; and group 3, bilateral-even, bilateral single mass of cement and also according to the presence of cement leakage as follows: posterior, paravertebral: anterior or lateral to the vertebral body, foraminal, and intravascular24) (Fig. 2). Follow-up radiography was performed at 6, 12, and 24 months after the procedure.
4. Statistical analysis
The SPSS version 12.0 statistical package was utilized for statistical analyses. Data were represented as mean┬▒standard deviation (SD) and p-values less than 0.05 were considered statistically significant. The Pearson correlation test was used to analyze the differences between the visual analogue scale (VAS) and other parameter changes, and the Kruskal-Wallis test was used to analyze the differences in radiological measurements at preoperation and postoperation, 6 months, 12 months, and 24 months.
RESULTS
Male to female patient ratio was 2:13. The mean age of the patients was 75.9 years (range, 55-90 years). The locations and numbers of the treated vertebrae were as follows: T7=1, T11=2, T12=2, L1=3, L2=3, L3=1, L4=2, L5=1. Mean T-score was -3.8 and mean amount of injected cement was 3.5 cc. The number of patients in group 1 was 4 (26.7%), group 2 was 6 (40.0%), and group 3 was 5 (33.3%). There were no cases of re-fracture at the surgical site, but fractures adjacent to the surgical site occurred in 3 cases (18.75%) and fractures remote to the surgical site occurred in 2 cases (13.3%) (Table 1).
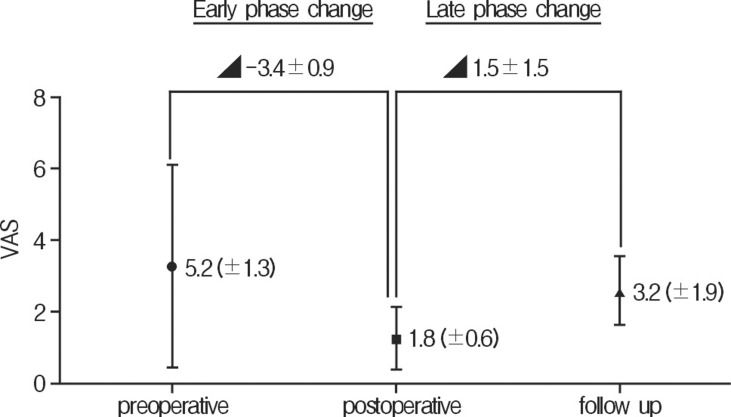
We investigated the relationship between bone factors (amount of PMMA and bone mineral density) and other factors. There was statistically significant correlation between amount of PMMA and follow up compression ratio (Table 2). Mean postoperative and 2-year follow-up of the VAS were 1.8 (┬▒0.6) and 3.2 (┬▒1.9), respectively (Fig. 3). However, there were no correlations between VAS and radiologic factor changes (Table 3).
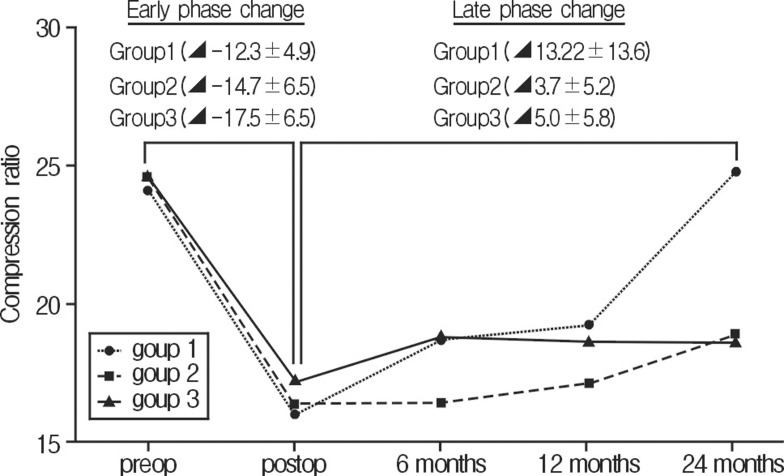
Total postoperative and 2-year follow-up compression mean ratios were -15.0% and 6.7%, respectively. Mean postoperative and 2-year follow-up changes in the compression ratio of the vertebral body height in group 1 were -12.3% and 13.25%, group 2 were -14.7% and 3.7%, and group 3 were -17.5% and 5.0%, respectively. The 2-year follow-up compression ratio was better in patients with even distribution of injected cement (group 2 and 3) than group 1. Unfortunately, it was not statistically insignificant (p>0.05) (Fig. 4).
Mean total postoperative and 2-year follow-up kyphotic angles were -3.6┬░ and 1.1┬░, respectively. Mean postoperative and 2-year follow-up changes in kyphotic angle in group 1 were -4.8┬░ and 2.2┬░, group 2 were -3.9┬░ and 0.75┬░, and group 3 were -2.35┬░ and 0.7┬░, respectively. The 2-year follow-up kyphotic angle was more aggravated in group 1 than in the other groups (p<0.05) (Fig. 5).
DISCUSSION
Percutaneous vertebroplasty involves injection of PMMA into a diseased vertebra. The use of vertebroplasty in the treatment of benign or malignant disease has been widely reported21,22,26). The effectiveness of percutaneous vertebroplasty in alleviating pain has been discussed comprehensively8,19). However, it has been reported previously that the degree of pain relief is not correlated with other factors such as the volume of injected cement, bone mineral density (BMD), and changes of the compression ratio and kyphotic angle2). In accordance with these studies, we also did not identify a relationship between these factors.
The optimal volume of injected cement is controversial13,14). The larger cement volumes are probably associated with greater risks of complications related to cement leakage, such as intradiscal leakage, epidural or neural foraminal compression, and pulmonary embolism7,25). Some studies reported that only 2 cc of cement was required to restore strength but that more cement was needed to restore stiffness14), but other studies reported that the magnitude of strength increase varied and was not correlated with the volume of cement injected13). Cement volume was also found to influence adjacent fractures, but less than 5 cc had little effect11,20). In the present study, we injected the cement in 2 aliquots of approximately 3.5 cc each.
Osteoporosis affects not only one part of the vertebral body but also the whole vertebra; therefore, it is important to stabilize the whole vertebral body. Furthermore, unipedicular distribution of cement in a vertebral body can promote single-sided load transfer and toggle (medial-lateral bending motion), which represents a biomechanically suboptimal result16,17). Therefore, uneven distribution of bone cement in the osteoporotic compression-fractured vertebral body has a risk of additional instability and concomitant danger of adjacent vertebral fractures. Therefore, even cement distribution is critical for long term stability and good outcome of the compressed vertebral body. Our data demonstrate a peri-interventional height gain of the vertebral body, a reduction in kyphotic angle, and an improvement of the compression indices during follow-up over 2 years, particularly in patients in group 3.
Vertebroplasty has been demonstrated to effectively reduce pain. The mean VAS score was 5.2 preoperatively, 1.8 postoperatively, and 3.2 at 2-year follow-up. It was shown that vertebroplasty achieved effective pain reduction in the postoperative period. Furthermore, the follow-up VAS score showed a tendency to increase again. In addition, radiologic findings such as compression ratio and kyphoitic angles showed us similar worsening with changes of VAS score. Therefore, we thought that, pain relief and stabilization of fractured spine in the immediate postoperative period is more significant effect of vertebroplasty. Therefore, we thought that, pain relief and stabilization of fractured spine in the immediate postoperative period is more significant effect of vertebroplasty.
Unfortunately, our study has some limitations. One is the retro-spective study which had been performed by several surgeons. The other is a small number of patients. Because we only included patients who underwent serial radiologic evaluations, we could only enroll the small number of patients. This study would be more valid and reliable if more patients performed serial radiologic evaluations were enrolled in this investigation.
CONCLUSION
Our study did not show a relationship between the clinical and radiologic results in vertebroplasty. The augmented spine tends to be more stable in cases with more even distribution of injected cement. Furthermore, vertebroplasty has a beneficial effect on pain relief and stabilization of fractured spine in the immediate postoperative stage.