Recurrent Spinal Meningioma: A Case Report
Article information
Abstract
Meningiomas are the second most common intradural spinal tumors accounting for 25% of all spinal tumors. Being a slow growing and invariably benign tumor, it responds favorably to surgical excision. In addition, spinal meningioma has low recurrence rates. However, we experienced a case of intradural extramedullary spinal meningioma which recurred 16 years after the initial surgery on a 64-year-old woman. She presented with progressive neurological symptoms and had a surgical history of removal of thoracic spinal meningioma 16 years ago due to bilateral low leg weakness. She underwent a second operation at the same site and a pale yellowish tumor was excised, which was histopathologically confirmed as meningothelial meningioma, compared with previously transitional type. she showed neurological recovery after the operation. We, therefore, report the good results of this recurrent intradural spinal meningioma case developed after 16 years with literature review.
INTRODUCTION
Meningiomas are the second most common intradural spinal tumors, accounting for 25% of all spinal tumors14). Being a slow growing and invariably benign tumor, it responds favorably to surgical excision. In addition, spinal meningioma has low recurrence rates. Risk factors for the disease recurrence after surgical excision have been discussed in many literature7,8,9,14). In this report, we describe a patient with intradural extramedullary spinal meningioma that recurred 16 years after the initial surgery.
CASE REPORT
A 64-year-old woman presented with weakness in both lower limbs, which had gradually progressed over the previous 4 months, and difficulty in walking on admission. She had no sensory dysfunctions or visceral involvements, but had a surgical history (the removal of thoracic spinal tumor) for a similar episode of bilateral lower leg weakness 16 years ago (Fig. 1).

Thoracic anteroposterior view showing total laminectomy state before second operation.
Clinical examination revealed a tender linear scar extending from the C7 to T9 spinous process. Neurological assessment revealed bilaterally increased muscle tone, associated with symmetrical paraparesis (3/5). No sensory loss or bladder/bowel involvement was evident. Magnetic resonance images revealed at Tl and T2; Godolinium enhanced image showed a well-enhanced tumor mass on the left side in the spinal canal and marked the compression of the spinal cord combined with compressive myelopathy (Fig. 2).
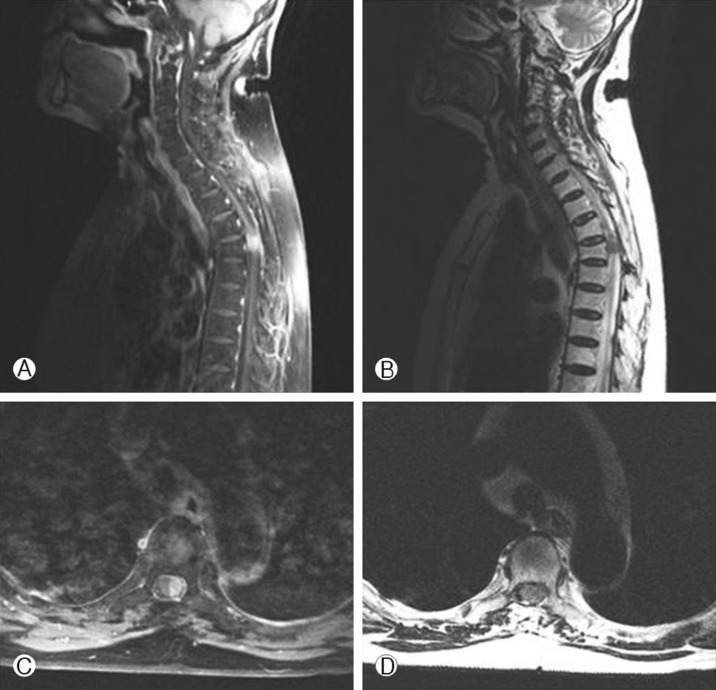
Gadolinium enhanced sagittal (A) and axial (C) magnetic resonance images showing the well enhanced tumor mass of left side in spinal canal and marked compression of the spinal cord. T2 weighted sagittal (B) and axial (D) magnetic resonance images of the affected region showing the tumor is posterior and left to the spinal cord.
She underwent a second surgery at the same site and a pale yellowish tumor was excised. The pathological examination confirmed that it was psammomatous meningioma (Fig. 3), compared with previously transitional type (microscopic examination showed nests or concentric whorls of menigothelilal cells revealing polygonal or oval cells with eosinophilic and indistinct bordered cytoplasm and round nuclei, also showing of frequent psammoma bodies in the center of the tumor whorls). The patient showed neurological recovery after the operation. Postoperatively, the patient's sensory parameters and bladder control improved. After 2 weeks, she showed a slight improvement of motor power and was discharged.

The neoplasm was wholly composed of calcified psammoma bodies with a few intervening fibroblastic cells (H&E, × 200).
DISCUSSION
Meningioma is a common type of tumor that accounts for 25-46% of spinal neoplasms8). The progress of spinal meningioma appeared to be more benign than its intracranial counterpart. Its prognosis is known to be favorable and the disease recurrence is also rare if the tumor is totally removed. In general, the reported rates of recurrence are ranged from 4% to 10%7,3,4,14). Most patients included in these recurrence results were older than 50 years. Furthermore, most results have been reported good functional outcomes in 74% to 85% of operated cases.
However, Cohen-Gadol et al.1) reported that a recurrence rate was as high as 22% in younger patients with age less than 50 years old. This study result showed that younger patients with the disease recurrence had aggressive histology, more extradural extension and longer follow-up periods. Therefore, younger age at the time of the first surgery could be a risk factor for recurrence in spinal meningioma.
Mirimanoff et al.8) reported that the recurrence free survival rates after total removal of meningioma during the follow-up periods of 5, 10 and 15 years were 93%, 80% and 68%, respectively. After subtotal removal of meningioma, the progression free rates were reported to be 63%, 45% and 9%, respectively, for the same follow- up periods. The most common histological features of spinal meningioma include meningotheliomatous, fibroblastic, transitional and psammomatous. Meningotheliomatous and psa- mmomatous types are reported to be histopathologically predominant4,6,8).
The other risk factors for the tumor recurrence are calcified meningioma and residual tumor remnants12). In a previous study, it was reported that histologically classified psammomatous meningioma had a low risk of aggressive growth and recurrence11). Doita et al.2) reported a case of psammomatous type of spinal meningioma which recurred 33 years after the surgery. In this case, a calcified recurrent spinal tumor was detected on a plain radiograph at the same site after an initial operation and preoperative paraplegia improved after the surgery.
Nadkarni et al.9) reported a similar case as ours, which described a recurrence 18 years after the initial surgery. It was revealed that the tumor was recurrent psammomatous meningioma. Surgical removal of the tumor resulted in complete neurological recovery9). It may suggest that psammomatous histological type associated with calcification is a risk factor for recurrent spinal meningioma. Our case was a histopathologically confirmed psammomatous meningioma which was a pathological variant most likely to be associated with calcification. However, no calcification was seen in preoperative radiography. Moreover, the first operation revealed that the tumor was a histologically transitional type with frequent psammoma body in the center of the tumor whorls. Therefore, contrary to the precedent reports in the literature, it is considered that psammomatous meningioma of our case have been transformed from the previous transitional type, of psammomatous types, to a calcification-associated psammomatous type when it recurred over the time. This suggests that the disease recurrence rate increases if histological calcification of meningioma is postoperatively manifested and if there are residual tumor remnants. This leads us to emphasize the importance postoperative histological re-examination to establish more active additional therapeutic strategies.
Spinal meningiomas were located laterally to the spinal cord or had a component that extended laterally. A posterior location was more frequent than an anterior one10). Unlike intracranial meningiomas, there was no correlation between recurrence and the resection of dural attachment and locations4,5). Although extradural attachment of spinal meningioma has not yet been determined as a cause of recurrence, a variety of spinal meningioma is shown to increase the rates of recurrence13,14).
CONCLUSION
Surgery is a preferred method in the treatment of spinal meningiomas owing to excellent functional improvements and low recurrence rates following surgery. Our patient has not shown any worsening of neurological symptoms during the follow-up period. A marked neurological improvement after the second surgery in this case implies that it is possible to achieve favorable surgical outcomes in the treatment of recurrent meningiomas. We intend to highlight that the factors leading to the recurrence of meningiomas after surgery include young age, subtotal re- section of the lesion, calcification and extradural attachment.