Cervical Expansive Laminoplasty with 90° Box-Shape Double Door Method
Article information
Abstract
Objective
The aim of this study is to introduce the surgical method with miniplate and compared the expansion rate of the spinal canal area with other kinds of lamina spacers.
Methods
Between June. 2008 and May 2011, we performed expansive cervical laminoplasty on 61 patients. We analyzed the results of these operations, examining type of lamina spacer used, spinal canal areas between pre- and postoperative CT scans, and operative methods.
Results
39 patients were analyzed retrospectively. Miniplates were used in 21 patients with 103 levels. Hydroxyapatite (HA) was used in 6 patients with 29 levels, and Centerpiece® was used in 12 patients with 54 levels. The expansion area was calculated using Photoshop CS3®. The expansion rate of the miniplates was 76.5%, that of HA was 49.8%, and that obtained with Centerpiece was 50.6%. The excellent 90° box-shaped widening of the laminae achieved through the surgery can be checked easily by AP X-ray. All miniplates are positioned horizontally and parallel, and the lamina is seen as a pedicle of thoracic or lumbar spine due to its 90° erect position. Neurologic improvement and clinical outcomes will be discussed. No complications were reported with miniplates.
Conclusion
Box-shaped laminoplasty with miniplates is the widest spinal canal expansion method among the three types of implants examined.
INTRODUCTION
Degenerative cervical spondylosis, herniated cervical disc, or ossification of the posterior longitudinal ligament (OPLL) can result in chronic compression of the spinal cord. Surgical treatment for this condition involves an anterior or posterior approach. Cervical posterior approaches for decompression, such as laminectomy and laminoplasty, are usually indicated for cervical myelopathy. Despite long-term doubts about its efficacy, cervical laminoplasty has gradually become established as an intervention for this condition3,5,19). Cervical expansive laminoplasty was originally carried out using the spinous processes as spacers. Since the design of classic open-door laminoplasty with the use of sutures, the procedure has been modified to reduce complications such as restenosis, axial symptoms, and segmental motor paralysis2). With the development of surgical implants, surgeons have begun to use various kinds of lamina spacers. We have used lamina spacers such as the spinous processes, hydroxyapatite (HA) spacers (Apaceram®), and Centerpiece®. Each method has its own advantages and disadvantages. The common purpose of all methods is, of course, to expand the narrowed spinal canal. However, there are little studies that compare the expansion rate of spinal canal area among spacers and we have felt that the aforementioned spacers do not always create enough space in some cases of severe spondylotic stenosis or OPLL. We therefore began to use the miniplate as a lamina spacer with the French-door method.
In this study, we introduce the surgical method for performing cervical laminoplasty with the miniplate, and compare the canal expansion rate among these methods with those attained using other types of lamina spacers.
MATERIALS AND METHODS
Between June 2008 and May 2011, we performed expansive cervical laminoplasty on 61 patients in Ilsan hospital. Among these patients, 39 underwent a postoperative CT scan. We performed a retrospective study of these 39 patients. We analyzed the surgical results, examining the type of lamina spacer used, difference in spinal canal areas between pre- and postoperative CT scans and operative methods.
1. Surgical techniques
The surgical procedure in the cases discussed here consisted of French-door (double-door) laminoplasty. Horizontal amputation of the spinous processes was performed and bilateral laminar exposure was carried out. Midline laminotomy was then performed with a drill, and lateral outer cortical bone drilling was done to facilitate elevation. When performing lateral outer cortical bone drilling, the surgeon must find the lamina-facet junction, which is a landmark for drilling. And it is important to drill just medial of facet joint to have enough spinal canal area. Because the narrow drilling space can induce the lamina fracture during elevating the lamina, adequate space is important to avoid the lamina fracture. After drilling, the ligament flavum was split centrally and each lamina and ligamentum flavum was opened bilaterally until the lamina stood straight. After proper positioning of the laminae, miniplates were applied to the space between both laminae. Intra-laminar drilling was performed for miniplate screw fixation. Usually, a miniplate is fixed with an approximately 8mm screw(Fig. 1).

In this patient, OPLL was extended from C4 to T1 (A). Double-door laminoplasty was performed (B). Apaceram was used in C4 and Miniplate was used from C5-T1 (C).
2. Methods of spinal canal measurement
We used Photoshop CS3® for measurement of the spinal canal area. The area of the preoperative spinal canal was defined as the region surrounded by the posterior border of the vertebral body and the inner border of the lamina, while that of the postoperative spinal canal was defined as the region surrounded by the posterior border of the vertebral body, the inner border of the lamina, and the inner border of a spacer. In cases of OPLL, OPLL was included in the spinal canal area as, if OPLL is excluded, the expansion rate can be overestimated. There are different ratios between the preoperative and postoperative CT scans. We have therefore adjusted the images to be the same size among the same sections and compared the number of pixels in the spinal canal. The canal expansion rate was calculated by the increase in pixels from the preoperative to the postoperative images (Fig. 2).
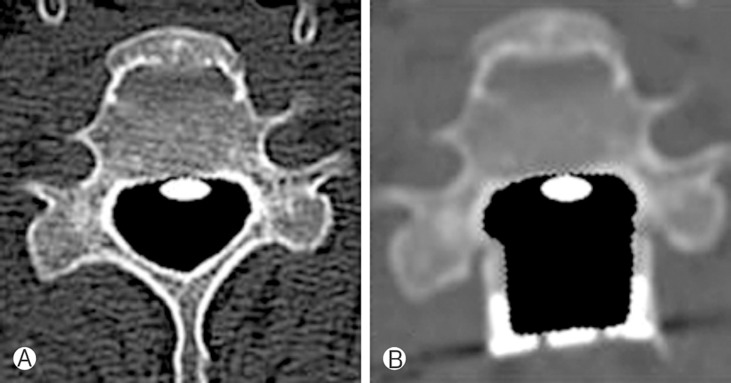
The preoperative CT scan (A) and postoperative CT scan (B) were compared. The spinal canal area included OPLL (white circle).
RESULTS
Among the 39 patients included in the study, 20 patients had OPLL and 19 had cervical spondylotic myelopathy (CSM). The mean age of the patients was 61.2 years (range 30-82). The male versus female ratio was 29:10. 39 patients were analyzed retrospectively (Table 1). Miniplates were used in 21 patients with 103 levels. HA was used in 6 patients with 29 levels, and Centerpiece® was employed in 12 patients with 54 levels (Table 2).

Characteristics of participants
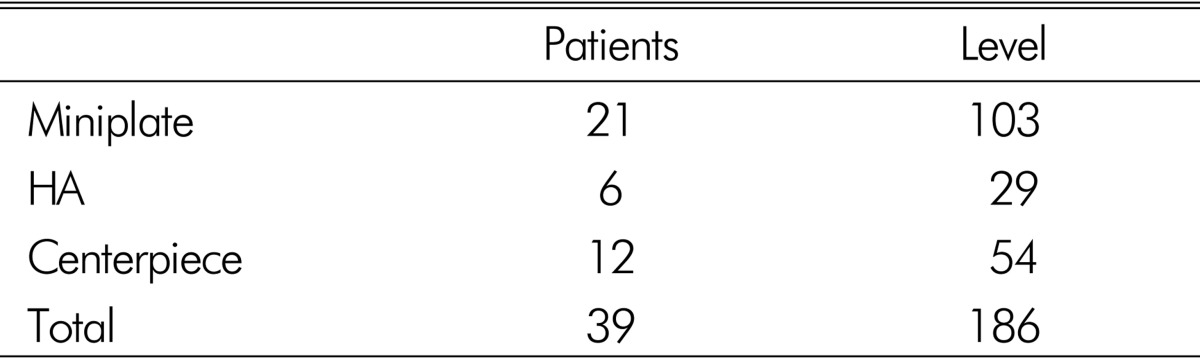
Patients and level for each surgery
The canal expansion rate with miniplates was 76.5%, that of HA was 49.8%, and that achieved with Centerpiece® was 50.6%. The canal expansion rate was highest when cervical laminoplasty was performed with miniplates (Fig. 3).
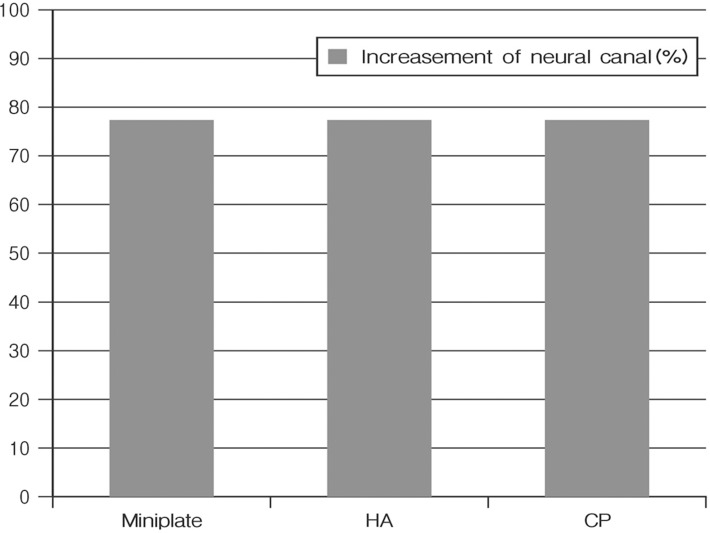
Increasement of neural canal in each groups
The excellent 90° box-shaped widening of the laminae achieved through the surgical procedure can be verified easily by AP X-ray (Fig. 4). All miniplates are positioned horizontally and parallel, and the laminae are seen like pedicles due to their 90° erect position.

Plain radiographs were taken for follow up. There is no kyphotic change after 6 months on plain radiograph.
Postoperative neck pain was found to be higher in the miniplate group than among those patients who received Centerpiece® or HA implants. Some patients complained of neck pain for as long as 1.5 months following the surgery. There were no reported complications related to the miniplates.
DISCUSSION
The incidence of degenerative cervical spondylosis, herniated cervical disc, and OPLL is increasing among the geriatric population. In these conditions, laminoplasty is considered the preferred surgical treatment. Numerous studies have reported satisfactory surgical outcomes with this procedure, and many technical modifications have been made12,13,18,20,21). Generally speaking, there are two types of laminoplasty methods. The first is the open-door method and the other is the double-door method. Double-door laminoplasty was originally devised by Kurokawa in Japan14,17,22). In this procedure, expansion of the spinal canal and preservation of the posterior structures for stability of the cervical spine are important16). Double-door laminoplasty allows easy placement of spacers and performance of bilateral decompression1,7,8,9,15,25).
There are not many studies that compare the spinal canal area among the different type of laminoplasty. Hirabayashi et al. reported that the open door laminoplasty with hydroxyapatite was significantly lager expansion ratio than the double door laminoplasty. In this study, however, we compared the amount of canal expansion among the three major types of implants used in laminoplasty. The major finding to come from this comparison is that box-shaped laminoplasty with miniplates allows the widest canal expansion of the three implant types. In addition, complications related to miniplates were not reported to occur.
1. Limitation in this study
Although we have confirmed that box-shaped laminoplasty with miniplates allows the widest canal expansion, there was no studies to examine clinical outcomes and radiologic changes.
The relationship between the degree of spinal canal expansion and clinical results after laminoplasty remains unclear. Itoh and Tsuji note that spinal cord function can be regained with a minimal degree of enlargement of the spinal canal and that a 4mm enlargement of the spinal canal is generally ideal11). Hamburger et al. report that patients with a postoperative cross-sectional area of >160mm2 achieve a better outcome4). Hirabayashi et al. believe that the optimal enlargement of the stenotic canal by laminoplasty is over 4-5mm in the sagittal diameter6). However, although the spinal canal area can be greatly increased during laminoplasty, excessive opening of the lamina may cause problems. Uematsu et al. report that kinking of the nerve root induced by maximal decompression may be related to the occurrence of postoperative C5 nerve root palsy and radiculopathy24). Excessive opening also creates epidural space and leads to the formation of more epidural scar tissue than expected10,23,24).
There is a need for additional studies to examine clinical outcomes and radiologic changes. Our study found no neurologic deterioration, severe pain, or radiological changes on X-ray, but it will be necessary to establish the standard for comparison, and long-term follow-up studies are required.
CONCLUSION
90° box-shaped double-door laminoplasty with miniplates is the widest spinal canal expansion method among the three implant types, and no complications related to miniplates were observed on short-term follow-up in this study. So if we use this method, we can expect to have maximal spinal cord decompression. However, wide-opening laminoplasty can induce some problems, such as epidural scar tissue formation and kyphosis. Therefore, we need to study more patients and additional long-term follow-up studies about clinical outcomes.