INTRODUCTION
Lumbar disc hernia is a frequently observed disease accompanied by lumbo and radiculopathy5). Radicular pain has been described for the first time by Dandy in 1929 as a clinical syndrome due to the extradural mass9). Mixter and Barr have proposed in 1934 that the extruded material may lead to sciatic pain and have described the surgical intervention to perform on the disc1). In literature, there are many studies showing the regression of huge disc hernia without surgical intervention5,8,13).
One of the most frequently observed diseases in spine is lumbar disc hernia. The correct patient selection is the most important factor affecting the result in lumbar disc surgery5). The priority treatment for lumbar disc hernia is conservative and neurological deficit, cauda equina syndrome are definitive surgical indications. Especially in disc hernia for lumbar regions, spontaneous regression is frequent and presents an 85% improvement in approximately 6 weeks11). Spontaneous disc regression is observed sometimes and is one of the important topics5). In our study, the spontaneous disc regression of a patient with huge lumbar disc hernia has been discussed in parallel with literature.
CASE REPORT
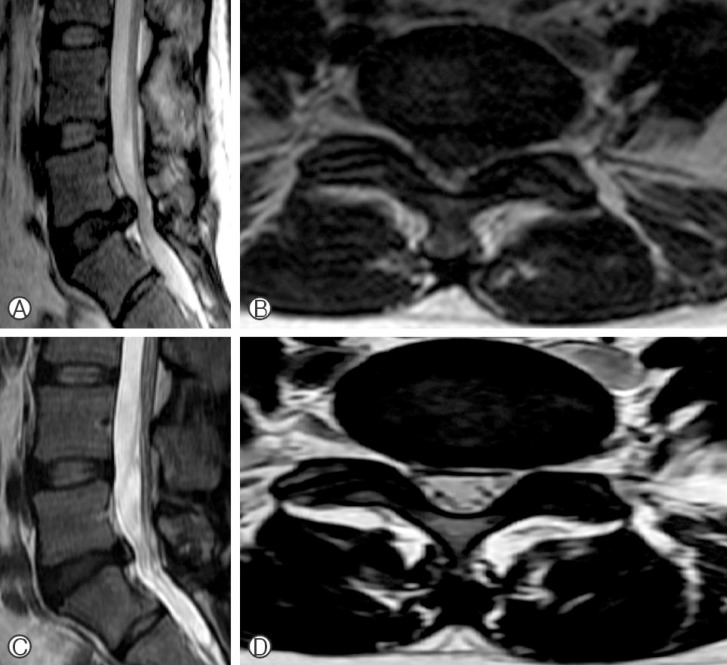
A fifty five year old female patient has applied to the polyclinic for backache and bilateral leg pain that developed upon stretching. The patient has been examined and has been evaluated together with a recently performed lumbar magnetic resonance imaging (MRI) film. It has been determined that she can be operated according to the complaints. However, as the patient said that a lumbar MRI has been performed 6 months ago, this film has also been evaluated. The patient has applied to another neurosurgery clinic for severe backache and bilateral leg pain 6 months ago and a surgical intervention has been proposed upon the diagnosis of sub-ligamentous huge disc hernia narrowing the spinal channel in the middle line at the L5-S1 disc in lumbar MRI (Fig. 1A, B). The patient who did not accept the operation and who affirmed that the pain has disappeared with medical treatment and physiotherapy has applied to our polyclinic for backache and leg pain. No pathology has been observed in the routine analyses performed. In neurological examination, the straight leg abduction test was free, and no motor and sensitive deficit has been detected. Her reflexes were normoactive. It has been observed on the new lumbar MRI that the disc hernia located at the L5-S1 disc interval has regressed spontaneously (Fig. 1C, D). It has been decided to perform a medical treatment and necessary recommendations have been proposed.
DISCUSSION
Disc hernia is one of the most frequent cause of radicular pain and backache. The spontaneous disc regression is usually in direct relation with clinic improvement and shall be confirmed with MRI images5).
Although the spontaneous regression of non-operated symptomatic disc hernia has been proposed, the mechanism has still not been determined clearly. First information about the spontaneous regression of disc hernia has been proposed in the 1980 by Guinta et al.3). Many papers have been published about this disease12).
Various hypotheses have been proposed about spontaneous disc regression. These have been described as dehydration, resorption with macrophage phagocytosis, retraction theory with the retraction of posterior longitudinal ligament, disc degeneration, and immunological reaction5,7).
In dehydration which is the first mechanism used to explain the spontaneous disc regression; the signal intensity of nucleus pulposus at the beginning of the hernia is higher than in original nucleus, and then it decreases with time, the hydration of nucleus pulposus at the beginning of the herniation is then rapidly followed by the dehydration of the nucleus pulposus6). As a result, nucleus pulposus loses water with time and then disappears by shrinking. The second mechanism is the resorption theory. The nucleus pulposus with hernia is considered as a foreign body by the body and the inflammatory process starts with neovascularization. The nucleus pulposus with hernia eliminated with enzymatic catabolism and phagocytosis. The third theory is the retraction theory with the retraction of the posterior longitudinal ligament. In herniation that is associated with the disc interval, it is the disappearing of disc material after the negativation of the pressure within the intradiscal space. The treatment modalities permitting the decrease of the intradiscal pressure in disc patients operate using this mechanism.
The type of disc herniation for spontaneous disc regression is more important than the dimensions of disc hernia. Moreover, there are studies defending that the presence of a transligamentous prolongation of the disc material with herniation is more important than sub-ligamentous and sequestrated herniation5). As well as studies proposing that the radiographic observations made on patients with sequestrated disc hernia show that this is more likely to undergo regression more rapidly compared to the other disc herniation sub-types14). In this study, it is possible to propose the regression as an inflammatory response against the free fragment. In addition, it has been declared in literature that even disc hernias that migrate to posterior epidural interval may undergo spontaneous regression4). The largest series about the regression of disc hernia in literature are those of Mart├Łnez-Qui├▒ones et al.7). In this study including 858 patients, the spontaneous disc regression in 33 patients has been detected by MRI11). In patients with sequestrated disc herniation and severe radicular pain, the regression of disc herniation shall be regularly monitored clinically and radiologically. The regression of sequestrated discs in these patients has been shown by 3-6 weeks monitoring and the control MRI performed between month 4 and 9 in a study of Orief et al.10). Moreover, there are also studies showing that the disc has regressed and that the patient has got better by conservative treatment in patients with huge disc herniation as in our patient2).
In the neurological examination of our patient, we have evaluated the straight leg abduction, motor and sensitive examination, deep tendon reflexes, the presence of atrophy and pathological reflexes. Straight leg abduction test is frequently observed in lumbar disc degeneration and spinal stenosis associated with lumbar disc degeneration13). We have used MRI for radiological examination in addition to routine laboratory analyses. The leucocyte, sedimentation, C reactive protein (CRP) and rheumatoid factor (RF) values of our patient were normal. Lumbar MRI observations supporting disc degeneration and dehydration were obtained in our patient. Usually accepted by everyone, disc herniation begins with disc degeneration, and most discs with herniation on T2 weighted MRI show 'black disc' low signal. Disc has pre-sented a hypointense aspect in all the T2 sections. These results have supported the dehydration of the disc. And this was compatible with spontaneous regression.
CONCLUSION
Although the spontaneous regression of disc hernia is a rare situation, it has been shown in many studies. However, data are limited to explain the spontaneous regression in lumbar disc disease. It is impossible to deny that the detection and the monitoring of the spontaneous regression of lumbar discopathy is possible using MRI. The loss of intensity in T2 sections in MRI supports the dehydration. No matter how the dimension of lumbar disc hernia is important, conservative treatment shall be preferred in patients with slight or middle neurological symptoms and observations, and shall be priority treatment 3-6 weeks before the surgery.