Lumbar Endoscopic Bony and Soft Tissue Decompression With the Hybridized Inside-Out Approach: A Review And Technical Note
Article information

Abstract
This study aimed to showcase the authors’ preferred technique of a hybrid of modern “inside-out” and “outside-in” endoscopic decompression. A case series of 411 patients consisting of 192 females (46.7%) and 219 males (53.3%) with an average age of 54.84 ± 16.32 years and an average of 43.2 ± 26.53 months are presented. Patients underwent surgery for low-grade spondylolisthesis (13 of 411, 3.2%), herniated disc (135 of 411, 32.8%), foraminal spinal stenosis (101 of 411, 24.6%), or a combination of the latter 2 conditions (162 of 411, 39.4%). The preoperative Oswestry Disability Index (ODI) and visual analogue scale (VAS) for leg pain were 49.8 ± 17.65 and 7.9 ± 1.55, respectively. Postoperative ODI and VAS leg were 12.2 ± 9.34 and 2.41 ± 5 1.55 at final follow-up (p < 0.0001). MacNab outcomes were excellent in 134 (32.6%), good in 228 (55.5%), fair in 40 (9.7%), and poor in 9 patients (2.2%), respectively. There was end-stage degenerative vacuum disc disease in 304 of the 411 patients (74%) of which had 37.5% had excellent and 50% good MacNab outcomes. Patients without vacuum discs had excellent and good 18.7% and 71.0% of the time. Direct visualization of pain generators in the epidural- and intradiscal space is the authors’ preferred transforaminal decompression technique and is supported by their reliable clinical outcomes.
INTRODUCTION
In the United States, endoscopic spinal surgery is being positioned by its prominent key opinion leaders to meet the need for simplified, less burdensome, and more cost-effective spinal decompression surgeries [1,2]. Strategies to deal with the increased demand for these types of procedures with the aging babyboomer population advancing into their retirement years is stressing the resource-strapped health care systems to a point where the stakeholders are being motivated to come up with better-valued solutions to avoid rationing of traditional open spine surgery [3,4]. Patients have also changed their stance on spine surgery seeking out spine surgeons who provide personalized spine care in the context relevant to the patients’ complaints at the time when the care is delivered by treating validated pain generators rather than basing decision for surgical treatment on traditional image-based criteria [5-9]. Instead, the authors have proposed for years a staged management approach limiting endoscopic spine care to the lumbar level to which the patients’ subjective weakness, and intermittent claudication limiting walking endurance and other physical activities can be traced back to [10]. These diagnostic and management strategies often lead to a unilateral or single-level foraminal stenotic process as a frequent source of pain [11,12].
Historically, the “inside-out” technique evolved based on the technology of contemporary spinal endoscopes available at the time [13,14]. Yeung et al. popularized the “inside-out” technique in 1998 in the United States and developed an entire platform of instruments around the Yeung Endoscopic Spine System YESSTM [15-22]. The “outside-in” technique was born in the late 1990ies as a result of Hoogland’s [23-25] curiosity and his advancement of the work predicated by Leu and colleagues [26-28], and the need to work inside the spinal canal and neuroforamen and not just in the confines of the intervertebral disc space [29-31]. Initially, the authors of this technique-oriented article supported by a video demonstration of their preferred contemporary transforaminal endoscopic decompression technique followed the “outside-in” method [29-31]. Over time, they adopted the hybridization of their “outside-in” [32] approach with the “inside-out” [33] technique to be able to directly visualize and treat painful degenerative pathologies in the posterior annulus anterior and directly located underneath the dural sac [6,33]. The “outside-in” method alone where the tip of the working cannula sits directly posterolateral to the dural sac in the neuroforamen has limited ability to deal with these painful pathologies for which reason the authors started to hybridize these 2 approaches to improve the reliability of these endoscopic spine surgery techniques and their associated clinical outcomes [33]. In the following, we describe the hybridized procedure in a step-by-step fashion.
TECHNIQUE DESCRIPTION AND DEMONSTRATIVE SURGICAL CASE
The surgical case example shown in the video accompanying this article (supplemental video clip 1) is of a 63-year-old female patient with symptomatic left-sided foraminal and lateral recess stenosis at the L4/5 level. The video is demonstrating the hybridized technique of initial outside-in decompression with an initial foraminoplasty to expose the triangular neuroforaminal safe zone before entering the intervertebral disc space utilizing the inside-out technique with the final position of the endoscopic working cannula being in between the intervertebral endplates. The patient consented for an outpatient transforaminal endoscopic decompression procedure.
1. Review the Preoperative Images
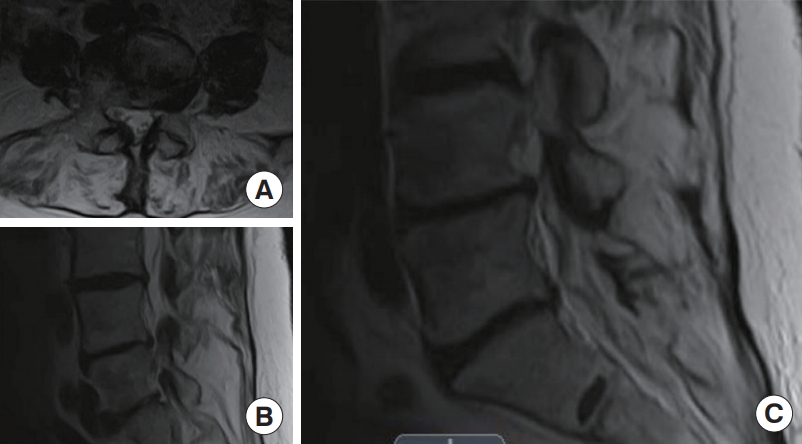
The preoperative radiographic film studies are reviewed in the posteroanterior and lateral views (Fig. 1) are studied from the presence of deformity, instability, and any other anatomical structure or factor that could obliterate or complicate the access to the surgical neuroforamen. These images should be reviewed for transitional anatomy, which should be taken into account for the planning of the attack angles and surgical approaches. The preoperative axial and sagittal magnetic resonance imaging scans through the surgical level (Fig. 2).

Posteroanterior (A) and lateral views (B) of the lumbar spine of a 63-year-old female patient with symptomatic leftsided foraminal and lateral recess stenosis at the L4/5 level who underwent transforaminal endoscopic transforaminal “outside-in” followed by “inside-out” decompression.
2. Positioning and Draping Patient
Record the positioning and draping of the patients with ergonomic setup of the tubing, cabling for the endoscopic decompression, watertight draping, and configuration of the video town and fluoroscopy unit.
3. Access Planning and Marking
In the posteroanterior (PA) fluoroscopy plane, record drawing of the midline along with the spinous processes. Draw out a curved line representing the location of the iliac wings. Draw a straight line representing the attack angle to the surgical neuroforamen in the PA plane (Fig. 3). Typically, at the L4/5 level, the distance from the midline is approximately 10 to 12 cm.
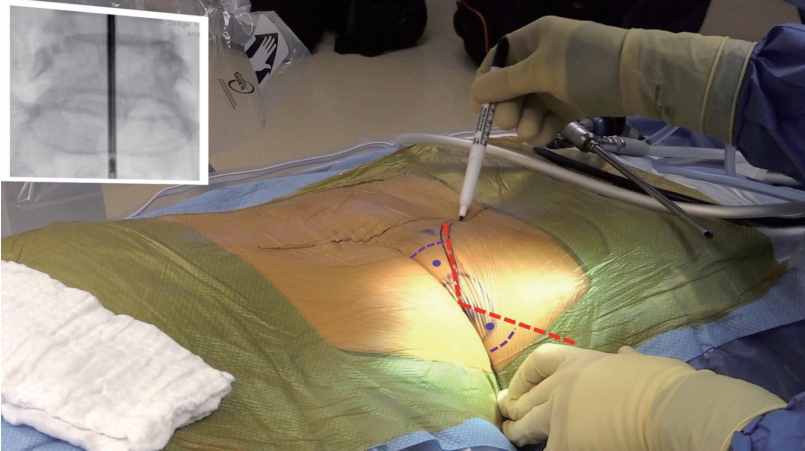
The patient in a prone position with both iliac crests drawn out (solid black line) and the black dotted line indicates the location of the spinous processes. The blue dotted line is drawn to connect the 2 posterior superior iliac spines and indicates an imaginary line drawn estimated to cross the L4/5 interspace.
In the lateral (LAT) projection, point the tip of the marker instrument at the posterior annulus of the surgical neuroforamen. Align the marker instrument to be in line with the intervertebral disc.
The access point is determined where the lines are drawn in the PA and LAT plane intersect. Attention: The complementary angles between the PA- and LAT-access lines and the perpendicular line drawn through the surgical intervertebral disc should be equal (Fig. 4).

Intraoperative view of the 63-year-old female patient discussed in Figs. 1 and 2 shown in prone position under posteroanterior (PA) fluoroscopy with a straight line drawn connecting the lumbar spinous processes. The ilium is drawn out on the approach side to help to place the access cannula. The most suitable access point can be estimated by drawing out trajectories on the PA and lateral (LAT) fluoroscopy images (red dashed line). Typically, the optimal location for the skin incision is where the 2 lines intersect (red dashed lines). The angles formed by these PA- and LAT-access trajectory lines form equal complementary angles (purple dashed lines and angle dot) with the horizontal line drawn across the surgical level.
4. Local Anesthesia and Monitored Anesthesia Care Sedation
Inject the skin entry point with 3–5 mL of 0.5% long-lasting 0.5% bupivacaine (Marcain, McKesson, Irving, TX, USA) with epinephrine to the extent of the duration of postoperative relief from incisional pain.
Advance an 18G 6-inch spinal needle onto the lateral aspect of the surgical facet joint and apply 2–4 mL of the same local anesthetic to the lateral aspect of the facet joint.
Introduce the spinal needle into the surgical neuroforamen and inject 1 mL of local anesthetic into the triangular safe zone onto the intervertebral disc. Before injecting, aspirate briefly to avoid intravenous injection.
5. Placement of the Working Cannula
The 18G 6-inch spinal needle is now advanced into the neuroforamen and positioned against the inferior pedicle.
A 300-mm guidewire is introduced through the spinal need, which is then withdrawn.
Three sequential dilators are not advanced into the neuroforamen over which then a 169-mm-long working cannula with a 45° bevel is then placed flush against the lateral aspect of the facet joint (Fig. 5) for best seal and a minimum spread of irrigation tissue in the surrounding tissues. The remainder of the surgery is typically done with the fluoroscopy unit positioned in the PA plane (Fig. 6).
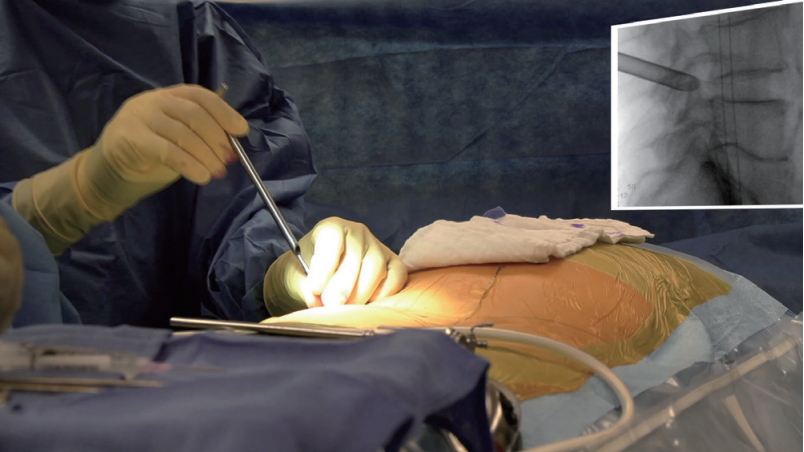
The beveled working cannula is placed on the lateral aspect of the L4/5 facet joint, as shown in the lateral intraoperative fluoroscopy projection.

6. Initial Foraminoplasty
The authors’ preference is to perform an initial foraminoplasty (Fig. 7) starting at the lateral aspect of the inferior pedicle sweeping up on the superior articular process to detach multifidus fibers, fat, facet joint capsule if needed, and foraminal ligaments to expose the triangular safe zone, and avoid any tethering of the exiting nerve root. The drill is advanced around the inferior pedicle by performing a limited pediculolectomy and drilling down any osteophytes from the ring apophysis impinging the traversing nerve root (Fig. 8).

The authors prefer an initial foraminoplasty with a low-speed (400 RPM), high-torque single-shafted, nonsheathed drill for rapid removal of bony- and soft tissue without causing a “white-out” effect from floating debris, or excessive bleeding due to the suction-vortex effect of the drill shaft spinning inside the oval working channel of the spinal endoscope.

The hand-held power drill is used to perform the majority of the foraminoplasty, including a small pediculectomy of the inferior pedicle and removal of common osteophytes of the ring apophysis typically located below the traversing nerve root. Once the tip of the 4-mm-round orbital drill bit has reached the lateral recess, the decompression of the traversing nerve root is typically complete. Drilling out the inferior portion of the neuroforamen by removing parts of the superior pedicle wall from lateral to medial also increases neuroforaminal volume.
The decompression of the traversing nerve root can be facilitated with a Kerrison rongeur (Fig. 9), which is best done by resecting bone from the posterior portion of the superior articular process, effectively raising the height of the lateral recess. Once completed, the neuroforamen is inspected, and the exiting nerve root and its dorsal root ganglion (DRG) are identified (Fig. 10A).

A 300-mm-long Kerrison rongeur with a 135° footplate is uniquely suited for raising the width of the lateral recess by egg-shelling out the superior articular process (SAP) and resecting the SAP from anterior to posterior (considering the patient is positioned in the prone position) effectively raising the roof of the lateral recess.

Several intraoperative endoscopic views are shown including (A) the endoscopic view after the initial foraminoplasty, (B) the initial decompression of the traversing nerve root with partial pediculectomy, (C) discectomy with the epidural fat shown in the right lower corner, and (D) ligamentum flavum in the left upper corner images of the traversing L5 nerve root, and (E) a view of the dural sac from below through an annular window after resection of a large contained central disc herniation. The last step can be achieved from the medialized resection of the disc herniation from the “outside-in” approach, or the “inside-out” approach from within the disc aiming upwards against the posterior annulus.
OUTSIDE-IN PORTION
1. Evaluating the Painful Pathology in the Epidural Space
After initial foraminoplasty and exposure of the triangular safe zone, the patient’s severe pathology is assessed.
This step includes the advancement of the beveled working cannula into the neuroforamen and to the lateral recess. A 360° view is taken, and painful anatomy is identified by palpation (Fig. 10B–D), intraoperative anesthetic injections, and provocative and analgesic chromo discography.
2. Target the Center of the Disc Space
A guidewire is introduced via the spinal needle advanced into the center of the lumbar intervertebral disc (Fig. 11).
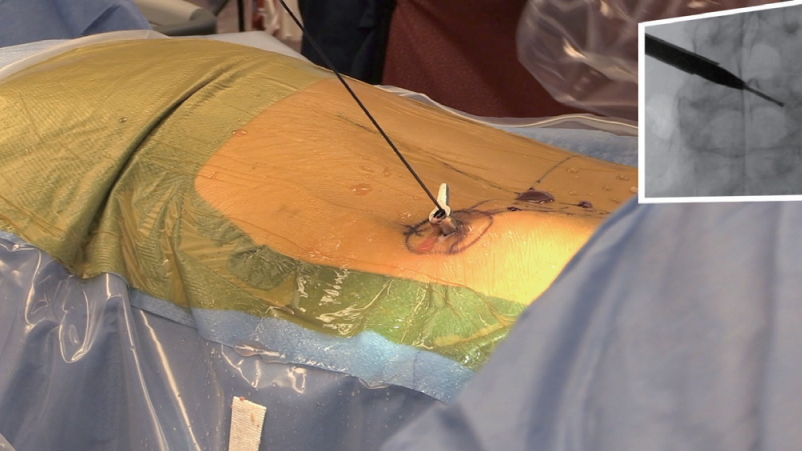
After the “outside-in” foraminoplasty and initial decompression of the traversing and exiting nerve roots as a result of discectomy, and inferior partial pediculectomy, the nitinol guidewire can be advanced into the intradiscal space. This is often done without difficulty in patients with end-stage vacuum degenerative disc disease, where the entire hollow disc space is accessible after initial discectomy. The working cannula is then advanced over the nitinol guidewire and a solid dilator into the disc space.
Sequential dilators are advanced into the center of the disc over which a Ø 8.9-mm working cannula is placed, allowing intradiscal inspection and removal of abnormal disc tissue (Fig. 12).

In the final step of the hybridized “inside-out/outside-in” approach to the interior of the intervertebral L4/5 disc, the working cannula is now within the disc space. It can be moved around in a systematic clockwise fashion to inspect the endplates, remove loose avital, and delaminated disc tissue from the interspace, and to remove large central contained disc herniations if present as in this case.
INSIDE-OUT PORTION
1. Discectomy
The intradiscal discectomy should be performed next in an attempt to remove any abnormal, avital, and delaminated disc tissue.
Any loose tissue should be removed in its entirety to facilitate visualization of the endplates and the posterior annulus.
2. Intradiscal Assessment of Painful Pathology
Beginning with the inspection of the posterior annulus, this team of authors prefers to perform a systematic inspection of the intervertebral disc space in a clockwise fashion. In case of the removal of a large central disc herniation, the dural sac can be inspected from below through an annular window (Fig. 10E).
This standardized choreography provides direct visualization of the posterior annulus, inferior, and superior endplate from one lateral recess to the other.
3. Wound Closure
Wound closure is done with a horizontal mattress stitch using 3-0 Monocryl without a drain.
4. Transfer Patient to Recovery Room
Enhanced anesthesia recovery protocols employed perioperatively allow for fast recovery and wakeup.
DISCHARGE AND POSTOPERATIVE REHABILITATION PROTOCOL
1. Before discharge home, the patients’ wounds and dressings are checked for any leakage since the authors do not use a drain routinely.
2. The patients are walked for a safety check within 30 minutes of their arrival in the recovery room.
3. A formal sign-out about the surgery and recovery is done with a family member, and the patient is discharged home.
4. Patients are discharged home from the ambulatory surgery center when they are comfortable, and a final neurological sensory and motor strength test is normal and within the expected from preoperative functioning.
5. Typically, patients are given a prescription for 10 tablets of 5-mg oxycodone and 2 mg of diazepam each for postoperative pain control to be taken as needed. They are instructed to use their nonsteroidal anti-inflammatory (NSAIDs) of choice or acetaminophen as well at their judgment to diminish the opiate use and its associated complications, including ileus, urinary retention, and others.
6. Patients are allowed to walk immediately with some weight lifting limitations of approximately 4.5 kg. in place. They are also instructed to avoid excessive bending or twisting at the waist.
7. Patients are instructed to give their body time to heal. They are discharged to wear the antithrombosis thrombo-embolic deterrent stocking until mobile enough at home. Patients are told that they may sleep either on their back, stomach, or side and that they can use pillows for support when lying on their side, place them behind their back and between their legs, or underneath their legs when on their back.
8. We suggest that patients change their position at least every hour when awake if they become uncomfortable to change their position and activity.
9. Patients are allowed to shower 5 days after surgery, or sooner as long as the incision is covered and kept dry. Baths, hot tubs or swimming pools are not permitted for 4 weeks.
10. Patients are instructed they should begin a walking program 2 to 3 days after surgery using the following schedule as a guideline:
• Day 1: Walk the length of the hallway at home 3–4 times, or walk to the end of the driveway and back once in the morning and again in the afternoon or evening.
• Day 2: Walk 1/2 block or the equivalent of a 1/2 block indoors earlier in the morning and again in the afternoon or evening.
• Day 3: Walk 1 block in the morning and again in the afternoon or evening.
• Day 4: Walk 2 blocks in the morning and again in the afternoon or evening.
• Day 5: Walk 3 blocks in the morning and again in the afternoon or evening. Continue increasing the distance you walk, as you are able. Let your comfort be your guide to how much you can do.
11. Once patients can comfortably sit, they are instructed to only a straight back chair such as a dining room chair or kitchen chair, and to increase the time & frequency they sit every day (example: 1st day, sit 3 times for 15 minutes each/2nd day 4 times for 20 minutes each/3rd day 5 times for 25 minutes, etc.). If there is pain after a few minutes, patients are told to get up and change positions.
12. Patients are seen in the office in close follow-up typically within 5 to 10 days for a wound check and consideration of a transforaminal epidural steroid injection if they show signs of a postoperative DRG irritation.
CASE SERIES
For this video illustration of the hybridized “outside-in” and “inside-out” procedure, the authors assembled an exemplary case series which consisted of 411 patients with an average age of 54.84 ± 16.32 years of which 192 of them (46.7%) were female, and the remaining 219 (53.3%) were male. These patients were followed for an average of 43.2 ± 26.53 months. The surgical indication was isolated herniated disc in 135 patients (32.8%), low-grade spondylolisthesis without translational motion on dynamic extension/flexion views in 13 patients (3.2%), spinal stenosis affecting the foramen and lateral recess in 101 patients (24.6%), and a combination of herniated disc and stenosis in the remaining 162 of patients (39.4%), respectively. As expected, the most common surgical level was L4/5 (201 of 411, 48.9%), followed by L5/S1 (113 of 411, 27.5%), and L3/4 (36 of 411, 8.8%). Most endoscopic surgeries were unilateral (385 of 411, 93.7%), and single-level surgeries (361 of 411, 87.83%). The disc herniations were subclassified as central in 167 patients (40.6%), paracentral in 124 patients (30.2%), or extraforaminal posterolateral in the remaining 120 of patients (29.2%). Primary outcome measure analysis showed significant reductions from an average preoperative Oswestry Disability Index (ODI) [34-40] score of 49.8 ± 17.65, and a visual analogue scale (VAS) leg [41] score of 7.9 ± 1.55 to an average postoperative ODI of 12.2 ± 9.34, and a VAS leg score to 2.41 ± 5 1.55 at final follow-up. The ODI and VAS reductions were 37.6 ± 16.98 and 5.49 ± 2.06, respectively, and were statistically significant (p < 0.0001). The analysis of the modified MacNab criteria [42,43] showed that 134 patients (32.6%) had excellent, 228 patients (55.5%) had good, 40 patients (9.7%) had fair, and the remaining 9 patients (2.2%) were rated to have poor outcomes. Of our 411 patients, 304 (74%) were found to have end-stage degenerative vacuum disc disease and the remaining 107 patients (26%). There was a statistically significantly higher proportion (p < 0.0001) of patients with excellent and good MacNab outcomes and the presence of a structurally defunct vacuum disc. Patients with vacuum disc had excellent and good 37.5% and 50% of the time, versus patients without vacuum discs who had excellent and good 18.7% and 71.0% of the time, respectively. The combined success rates are nearly equivalent at 87.5% (vacuum disc present), and 89.7%.
DISCUSSION
The hybridized version of transforaminal endoscopy consisting of an initial “outside-in” approach with decompression in the epidural space followed by the intradiscal “inside-out” decompression under direct visualization is a result of years of outcome research recently published by the authors [3,33]. Fiveyear follow-up data clearly showed lower reoperation rates if the “inside-out” treatment of intradiscal pain generators was included in the transforaminal decompression surgery [33]. Consequently, the authors started combining the 2 techniques sometimes in different order of steps but eventually arriving at the same end-result–a combined “outside-in” and “inside-out” endoscopic decompression procedure to treat pain generators in the epidural space as well as inside the disease intervertebral disc.
To the novice surgeon who is deciding on entering the field of spinal endoscopy and seemingly has to choose between the 2 techniques, the fundamental difference between them is often not immediately evident [6]. The apparent difference is the initial location of the working cannula. For example, when a surgeon employs the “inside-out” method, the posterior annulus under the dural sac may be directly visualized [15]. This portion of the posterior annulus cannot be visualized with the “outside-in” method, where the tip of the working cannula sits directly posterolateral to the dural sac in the neuroforamen. The 2 fundamental differences in cannula position determine what the surgeon can initially see, evaluate, and treat endoscopically. Intraoperative confirmation of suspected pain generators may be done in the awake, yet sedated patient where provocative or analgesic testing with disco- and epidurography may aid in their correct identification. The most commonly visualized painful epidural conditions may range from (1) inflamed disc; (2) inflamed nerve; (3) hypervascular scar; (4) hypertrophied superior articular process and ligamentum flavum; (5) tender capsule; (6) impacting facet margin; (7) superior foraminal facet osteophyte; (8) superior foraminal ligament impingement; to (9) a hidden shoulder osteophyte, (10) autonomic, (11) synovial cysts, and (12) furcal nerves, or conjoined nerves. Intradiscal pain generators include medial annular tears and unstable disc fragments delaminated from the endplates, devitalized detached disc tissue [16].
In the authors, opinion the ability to turn the opening of the working cannular towards the posterior annulus and to enter the epidural space through an annular window once the discectomy, including an annular resection, is completed is likely the most misunderstood aspect of the “inside-out” method. The annular window technique affords the surgeon the ability to adequately decompress the neural elements by removing bony osteophytes indenting the dural sac from below, or pain generators residing within the annulus itself from the approach side to the opposite lateral recess if needed. In other words, there are few limitations of the inside-out technique to treat painful conditions in the epidural space by way of the annular window technique if executed expertly. This expanded view of the anterior lumbar epidural space is unique to the “inside-out” technique. This hybrid of “outside-in” and “inside-out” may offer the surgeon the ability to perform a complete evaluation of the pain generators within the symptomatic lumbar motion segment and is to the authors of this article a more obvious choice in patients with advanced degenerative disc disease. In the older patients, end-stage degenerative vacuum disc disease is routinely found during lumbar transforaminal endoscopy in up to 73% of patients over age 45, where there often is a collapsed vacuum disc without any structural integrity [44-48]. In those patients, an “inside-out” look inside the disc is a sensible step that provides more reliable long-term outcomes with fewer revision surgeries. In younger patients, the authors are concerned with the propagation of progressive vertical disc collapse with the “inside-out” technique for which reason they routinely start the transforaminal decompression with the “outside-in” technique and only enter the intervertebral disc space if there is lack of structural integrity to improve outcomes.
Many newer approaches and technique variations have emerged as a result of improved surgeon skill level, technological advances, and better motorized endoscopic decompression tools. Examples include the foraminoplasty or facetectomy decompression technique with outside-in spinal stenosis decompression and the mobile “outside-in” technique. Kim et al. [49] recently publicized the latter method. A novel technique is distinct from the traditional “outside-in” and “inside-out” concepts as it relies on a precise landing within the foramen in a mobile manner and does not solely depend upon the foraminoplasty to gain access to the lateral recess and the spinal canal. This newer technique as the hybridization approach of the “outside-in” and the “inside-out” presented by the authors in herein are representative of spine surgeons’ ongoing quest to improve upon their existing protocols to solve problems that they encounter with contemporary endoscopic spinal surgery techniques as they attempt to treat more complex issues due to severe canal compromise and high migration while advancing the endoscopic spinal surgery patient care agenda. The staged management approach [10] advocated for by the authors leads to highest patients’ satisfaction with their clinical outcomes particularly when the final determination of the plan of care of their multilevel degenerative lumbar spine process is a shared decision between patient and provider based on a complex analysis of each patient’s painful patho-anatomy [16,19,49-53].
Notes
The authors have nothing to disclose. This manuscript is not meant for or intended to endorse any products or push any other agenda other than the associated clinical outcomes with endoscopic spine surgery. The motive for compiling this clinically relevant information is by no means created and/or correlated to directly enrich anyone due to its publication. This publication was intended to substantiate contemporary endoscopic spinal surgery concepts to facilitate technology.
SUPPLEMENTARY MATERIALS
Supplementary video clip 1 can be found via https://doi.org/10.14245/ns.2040160.080.v.1.