INTRODUCTION
Cervical myelopathy is often associated with rigid kyphosis. It is known to adversely affect the progression of myelopathy [1] and neck function [2]. Furthermore, severe kyphosis is often accompanied with K-line negative, which indicates a sufficient posterior shift of the spinal cord and neurologic improvement could not be obtained after posterior decompression surgery. Therefore, surgeons should consider simultaneously correcting the deformity and decompressing the neural tissue. However, this is surgically demanding. Posterior laminectomy and fusion can restore cervical lordosis when the deformity is flexible. However, it is not possible to restore cervical lordosis when the deformity rigid as the posterior drift of the spinal cord does not occur [3-5]. Anterior cervical corpectomy and fusion (ACCF) has been widely used for direct decompression as treatment for multilevel myelopathy, but high rates of implant dislodgement due to graft instability and dural tear during resection of the vertebral body have been reported, especially in patients with ossification of the posterior longitudinal ligament (OPLL) [6-9]. Hence, we previously reported a novel anterior decompression technique called vertebral body sliding osteotomy (VBSO) [10-13].
VBSO allows for expansion of the spinal canal by anteriorly translating the vertebral body without complete removal. Our previous studies demonstrated that VBSO can decrease the risks of dural tear and pseudarthrosis while effectively achieving cord decompression. In addition to adequate decompression, its superior outcome with restoration of cervical lordosis and improvement in sagittal alignment has been reported [11]. Improvement of segmental and global cervical lordosis is greater in VBSO than in ACCF after surgery. Moreover, maintenance or improvement of lordosis after VBSO compared with those after ACCF was confirmed in our previous study.
Improvements of sagittal balance and cervical lordosis are crucial for better surgical outcomes such as maintenance of forward gazing, pain relief, and fewer problems at the adjacent level [14-16]. Herein, we review the effectiveness of VBSO for the correction of kyphosis and present a technical note on VBSO to aid surgeons in performing deformity correction and anterior decompression safely and efficiently in patients with severe kyphosis and cervical spondylotic myelopathy.
ILLUSTRATIVE CASE
This study was approved by the Institutional Review Board of Asan Medical Center (S2020-2041-0001). Written informed consent was obtained from the patient for the publication of this case and any accompanying images. A 59-year-old woman presented severe neck pain, weakness of both upper extremities, and gait disturbance. Her neck and radicular arm pains had visual analogue scale (VAS) scores of 7 and 8/4, respectively. The neck pain and stiffness had started long before. She had a > 35-year history of rheumatoid arthritis with medication and developed severe osteoporosis because of the prolonged corticosteroid medication (T-score, -4.2). For the past 4 months, she had been experiencing progressive weakness, tingling, and clumsiness in both hands. In addition, she presented with subjective weakness in walking. She had moderate limitations of neck motion in all directions. She demonstrated diffuse weakness of the upper extremities, with marked weakness of elevation of both shoulders (grade 3), elbow flexion (grade 3), and elbow extension (grade 3). Her deep tendon reflexes in the lower extremities were exaggerated. Hoffman and Babinski signs were positive bilaterally.
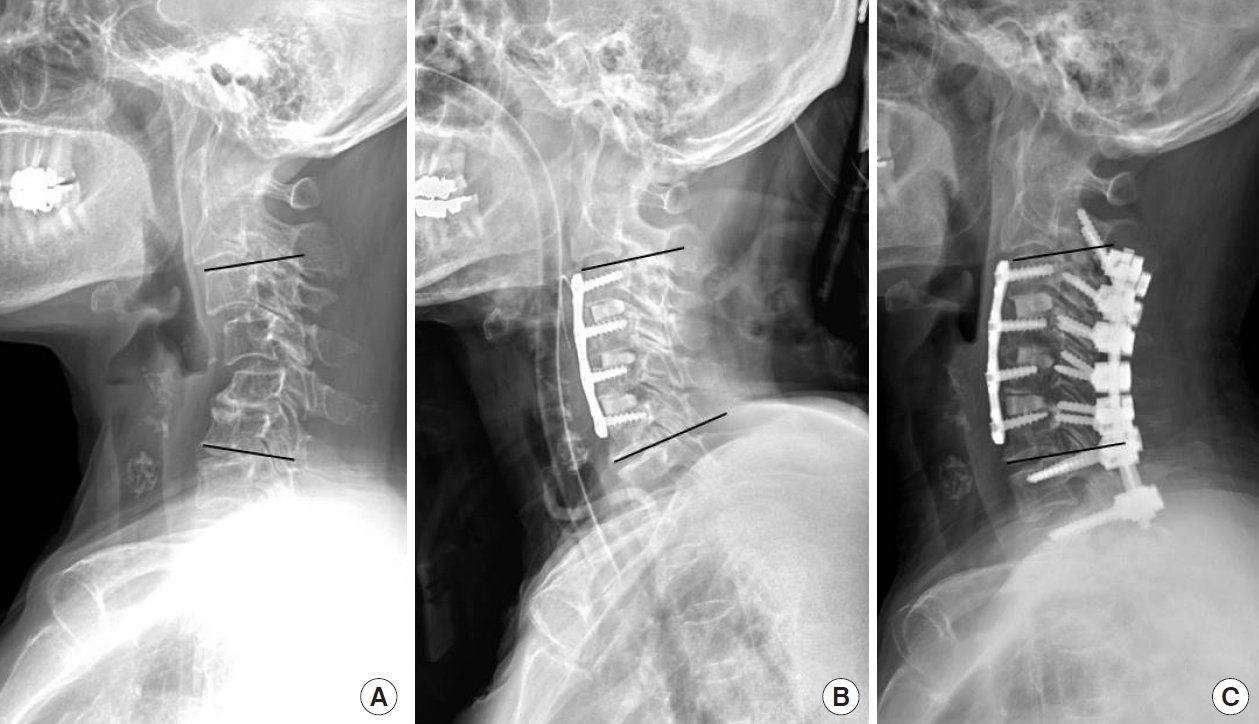
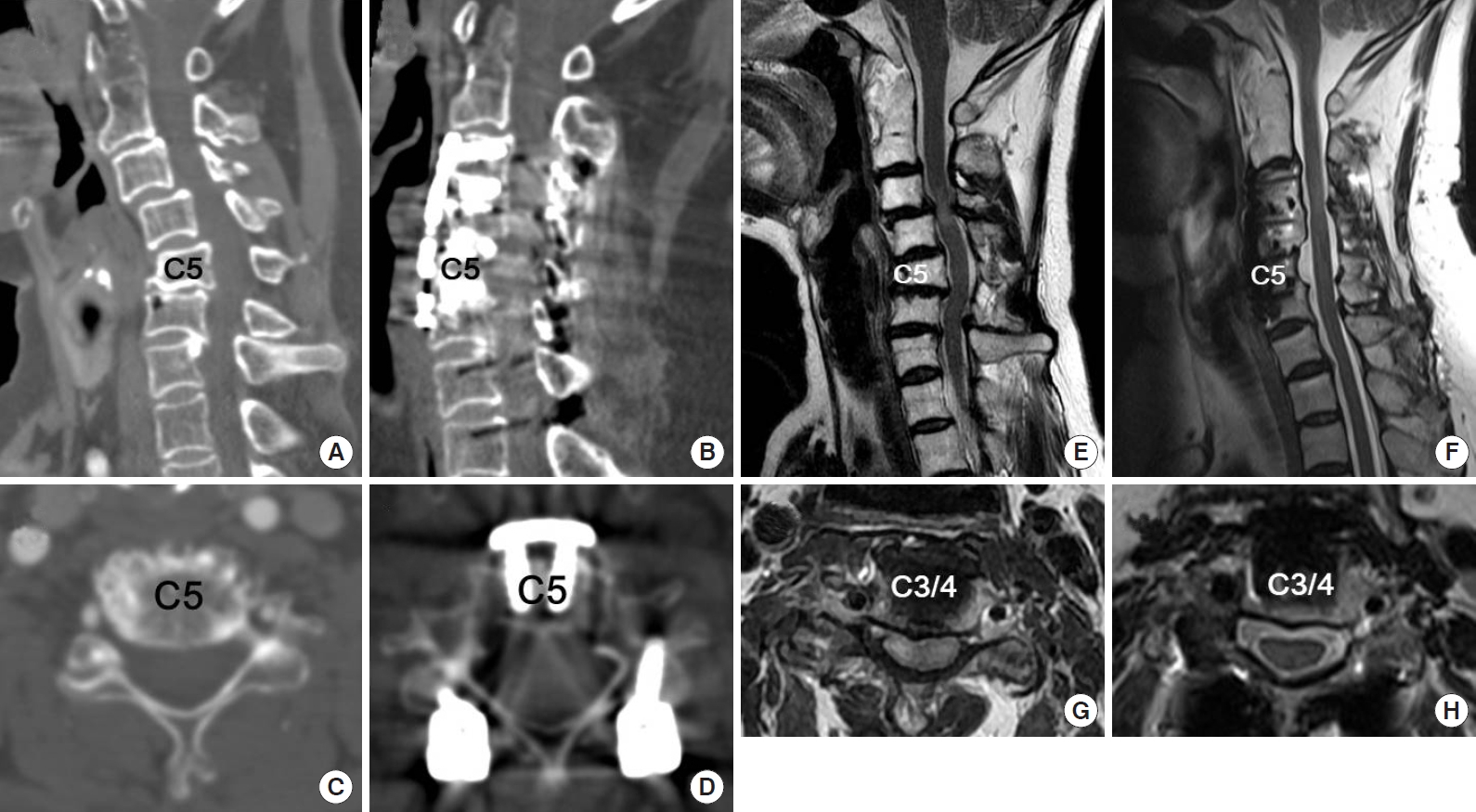
Plain radiographies of the cervical spine revealed the following: marked narrowing of the intervertebral disc spaces; marked anterior and lateral formations of osteophytes; staircase deformity of C3ŌĆō5; and a regional angle between C3 and C6 of 22┬░ of kyphosis (Fig. 1). Magnetic resonance imaging (MRI) of the cervical spine demonstrated severe central stenosis at C3ŌĆō4, with stenosis of both foramina at C3ŌĆō4, C4ŌĆō5, and C5ŌĆō6. Cord signal change was also noted.
The patient underwent anterior cervical decompression and fusion (ACDF) at C3ŌĆō6 with VBSO at C4 and C5. She had severe osteoporosis (T-score, -4.2). Further, additional posterior instrumentation was performed because we thought that anterior plating was insufficient to hold the correction of kyphosis. The preoperative VAS scores for the neck and arm pains decreased from 7 and 8/4 to 3 and 5/3 after operation, respectively. The weakness of the upper extremities also recovered gradually to grade 4 within 6 months after the operation. The regional angle between C3 and C6 improved by 34┬░ to 12┬░ of lordosis and was maintained at 7┬░ at 1 year after operation. Postoperative MRI and computed tomography (CT) revealed satisfactory decompression of the central canal stenosis, improved foraminal stenosis at C3ŌĆō4, C4ŌĆō5, and C5ŌĆō6, and solid fusion (Fig. 2). Flexion and extension dynamic lateral plain radiographies also revealed no instability and pseudarthrosis.
SURGICAL TECHNIQUE
Please see the Supplementary video clip 1 for a video of the procedure.
1. Multilevel Discectomy and Uncinate Process Resection
A standard Smith-Robinson approach through a transverse or longitudinal incision to the anterior cervical spine is performed. Lateral elevation of the longus coli is performed just lateral to the uncinate process. After soft tissue dissection, the appropriate surgical level is confirmed using a portable image intensifier. Initially, multilevel discectomy is performed at the superior and inferior levels of all the involved vertebral bodies. The involved level is defined as one disc space cranial and caudal to the mass when the mass is associated with the OPLL. After complete discectomy, resection of the uncinate processes is performed if decompression is necessary for the foraminal stenosis. Removing the uncinate processes makes the width of the mobile fragments of the vertebral bodies wider and decompresses the foramina.
2. Resection of the Posterior Longitudinal Ligament at the Most Cranial and Caudal Disc Levels
The posterior longitudinal ligament (PLL) at the discectomy level is resected using a Kerrison punch to reduce the resistance against the free anterior translation of the vertebral bodies. However, the PLLs between the involved levels, which will be translated, do not need to be released.
3. Mobilization of the Vertebral Body Fragments
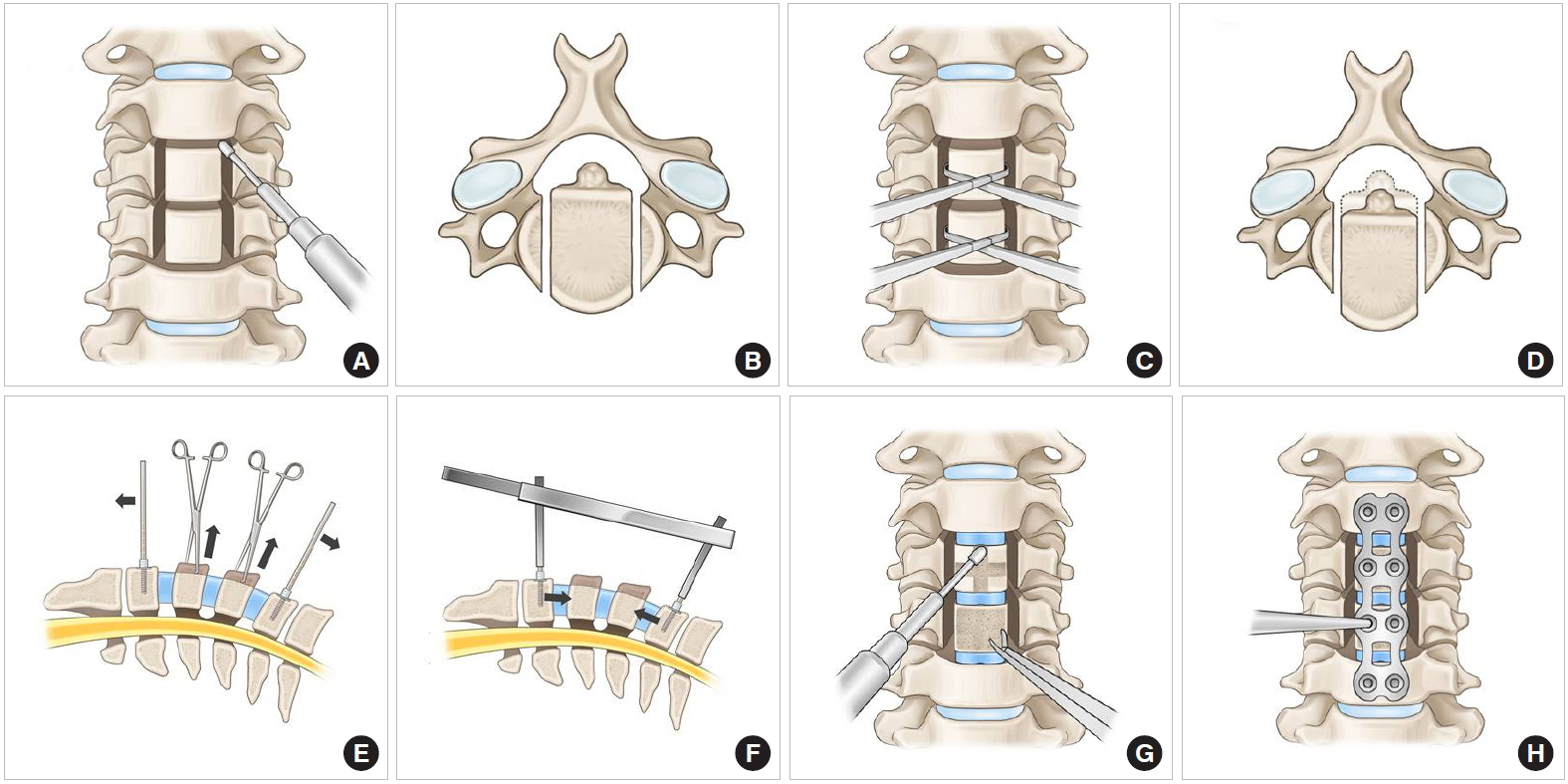
Two parallel longitudinal slits are made along the medial borders of the uncinated processes by using a 2- to 3-mm high-speed burr (Fig. 3A, B). For 2-level VBSO, longitudinal incision and 2 self-retractors in succession might be helpful to secure sufficient surgical field. Subsequently, the slits are deepened quickly to the posterior wall of the vertebral bodies. The posterior wall of the vertebral bodies is trimmed to cut the vertebral bodies into a box-shaped mobile segment. Cutting by Kerrison punch is not recommended because it frequently results in bleeding. Caspar pins should be placed into the vertebral bodies above and below the desired level with distraction before mobilizing the vertebral body fragments.
4. Anterior Sliding of the Vertebral Bodies
Allis forceps are used to grab each mobilized vertebral body. Gentle anterior traction is applied to the vertebral bodies. Some up-and-down wagging motions could help to release the central fragment and make it more mobile (Fig. 3C, D). Through preoperative measurement of the anteroposterior diameter of the OPLL on CT images, the extent of anterior sliding that is needed is estimated in advance. After pulling out the mobile fragments with the OPLL or disc masses, successful anterior translation is confirmed by comparing the height of the protruding anterior portion of the vertebral bodies and the anteroposterior diameter measured before surgery.
5. Anterior Column Reconstruction With Interbody Cage Insertion
Cervical interbody cages are packed with locally harvested bony fragments during discectomy and foraminotomy. Cage size and angle can be freely selected on the basis of the height of the disc space with consideration of the physiological sagittal alignment. Through a properly sized cage insertion, the cervical anterior column is temporarily stabilized for the next procedure by releasing the traction force made by a Caspar retractor (Fig. 3E, F).
6. Resection of the Protruding Anterior Vertebral Bodies and Cervical Plating
The protruding portions of the anteriorly translated bodies are shaved down using a high-speed burr or Leksell rongeurs (Fig. 3G) before applying anterior plating to enhance stability. When shaving down the anteriorly translated vertebral bodies with a high-speed burr, care must be taken not to push the anteriorly translated fragments back. The plate should be bent to fit the target sagittal alignment before placing. For additional anterior translation of the mobilized vertebral bodies due to the lag screw effect, screws are inserted, gradually tightening them after proper drilling and tapping (Fig. 3H). Local bone dust is packed additionally into the disc space and lateral slits. Meticulous hemostasis is achieved using hemostatic materials. Using the intraoperative image intensifier, appropriate migration of the vertebral bodies is confirmed by checking the location of the posterior margins of the involved vertebral bodies.
DISCUSSION
Restoration of cervical lordosis in patients with deformed cervical myelopathy is important for better neurological outcomes, forward gaze, decreasing axial pain after surgery, and vertebral artery hemodynamics because of the stretched vertebral artery course [2,17]. Restoration of the segmental sagittal alignment is related to notable improvement in the 36-Item Short Form Health Survey physical component scores, and the severity of disability increases with positive sagittal malalignment after surgery [18]. The segmental sagittal angle affects the C2ŌĆō7 lordosis and is related to the C0ŌĆō2 lordosis and T1 slope. Lee et al. [16,19] demonstrated that surgical correction of cervical kyphosis affects the T1 slope and indicates that restoration of the cervical lordosis increased the thoracic kyphosis, converting it into a physiological curve. According to their results, decreased thoracic kyphosis from cervical kyphosis might increase the unnecessary energy consumption for maintaining posture and a comfortable horizontal gaze. Therefore, restoration of the cervical lordosis should be considered especially in patients with severe deformities who have axial neck pain and myelopathy symptoms.
In patients with adequate cervical lordosis, posterior decompression surgery is commonly used. However, laminoplasty cannot improve symptoms sufficiently in patients with K-line negative cervical myelopathy. Most patients with kyphotic deformity and myelopathy are classified as K-line negative. The treatment algorithm for cervical myelopathy is illustrated by a flow diagram (Fig. 4). The advantage and disadvantage of the posterior approach for K-line negative deformities were wellexplained in previous studies [3,20,21]. Laminoplasty frequently induces progression of the OPLL, compared with fusion surgery, and young patients with mixed or continuous types of ossification face a higher risk of progression after surgery [22,23]. In addition, laminoplasty is known to be associated with aggravation of kyphosis [4]. Furthermore, neurological improvement cannot be obtained with posterior decompression alone in patients with K-line negative cervical myelopathy [3,24,25]. Another problem is sustained axial pain after posterior cervical spine surgery, which is related to the detachment of the semispinalis cervicis muscle and reconstruction of the extensor musculature [26].
ACCF has been widely used for direct decompression as a treatment of multilevel myelopathy. However, ACCF is technically demanding and requires perioperative management of troublesome complications, including cerebrospinal leakages and graft-related complications [27]. Sasso et al. [28] reported a complication rate of 69% and reoperation rate of 24% when the ACCF was performed at > 3 levels. We previously reported a novel technique, namely, VBSO, as a replacement for ACCF in the treatment of OPLL myelopathy [10-12]. VBSO was developed in 2012 by our first author and introduced in 2013 at the Cervical Spine Research Society (CSRS)-Asia Pacific and the Korean Society of Spine Surgery. Minimum 1-year follow-up data were also presented in the CSRS annual meeting in 2014 [29]. After accumulating enough cases, we presented several articles that demonstrated the objective safety and efficacy of the technique [10-13]. Meanwhile, a similar technique was introduced in Asia, but we believe the originality of this technique belongs to us.
In VBSO, the vertebral body is translated anteriorly to widen the spinal canal, minimizing the need for direct manipulation of the interspace between the PLL and dura mater, or complete removal of the involved vertebral bodies. [13] It shows fewer complications, as it minimizes the direct separation of the PLL from the dura. Thus, it can notably reduce the risk of dural tears. However, translation alone might cause dural tear in severe adhesion between the PLL and dura mater; hence, caution might be needed in these cases. Pseudarthrosis after fusion surgery through an anterior approach can be a major concern, and its incidence increases with fusion of multiple levels and severe deformities. Patients who experience migration of graft materials, loosening of metallic implants, or severe axial neck pain associated with nonunion and/or evidence of vertebral column instability may require revision surgery. Our previous study showed that VBSO was superior than ACCF in terms of less pseudarthrosis and pseudo-motion [28,30,31]. The solid fusion after VBSO is thought to be achieved more easily by the early formation of bridging bone along the longitudinal slits.
VBSO showed better outcomes than ACCF in terms of canal widening and improvements of myelopathic symptoms [13]. Therefore, the VBSO technique is an effective and safe option for anterior decompression surgery in patients with cervical myelopathy. In addition to its safety and efficiency of proper decompression and fusion, VBSO can be a powerful method to restore cervical lordosis [9]. As VBSO is based on multi-level ACDF, it is more favorable than ACCF for restoring cervical lordosis [11]. In addition, it can reconstruct the target alignment and smooth curvature in cervical lordosis because the multiple placement of various-sized lordotic interbody implants at each level has benefits over multilevel corpectomy and fusion using a single long-distance graft by distributing the load more evenly. The high degree of lordotic restoration using VBSO can be explained by its procedure. Anterior column reconstruction consists of the anteriorly translated vertebral body, maintained multilevel interbody cage in a very anterior column, and resection of multiple levels of posterior vertebrae. Moreover, the fact that the extent of correction can be controlled makes VBSO a powerful tool. Acute restoration of cervical lordosis may induce ligament flavum buckling to prevent the canal widening effect. However, restoration of disc space height during the VBSO procedure could minimize this risk. Furthermore, as the powerful widening effect of VBSO is even better than that of ACCF, neurological improvement was known to better with VBSO than with ACCF or anterior floating methods. In our previous studies, segmental lordosis in ACCF decreased at the final follow-up as compared with the postoperative values [11]. On the other hand, the segmental lordosis in VBSO even increased at the final follow-up. This could be explained by the greater number of preserved endplates of the vertebral bodies providing structural support to prevent graft subsidence than that in ACCF. Concerning the mechanical support to maintain segmental lordosis, VBSO is more stable than ACCF because surgeons could place more screws [11]. Therefore, VBSO can improve cervical lordosis in patients with cervical spondylotic myelopathy and kyphosis because multiple ACDFs above and below the VBSO level increase the cervical lordosis more effectively, and the preserved vertebral bodies in VBSO provides structural support. If patients who need revision surgery who have undergone laminoplasty develop kyphosis progression, VBSO may be a reliable treatment option to restore cervical lordosis with additional anterior decompression.
CONCLUSION
VBSO is a feasible treatment option for cervical myelopathy with rigid kyphosis. It improves cervical lordosis in myelopathy patients with kyphosis because the multiple ACDFs above and below the VBSO level increase the lordosis effectively. It is also a safe and effective technique for anterior decompression in patients with multilevel cervical myelopathy in terms of solid fusion, and lower rate of complications, including dural tear, pseudarthrosis, and graft dislodgement.