INTRODUCTION
The essential mechanical factor of cord tethering is that any of the inelastic structures fastening the caudal end of the spinal cord produce traction effects on the lumbosacral cord32,35). Most of the conditions resulting in tethered cord syndrome (TCS) are congenital. This syndrome may be closely associated with spina bifida, tight filum terminale, lipomeningomyelocele, split cord malformations, dermal sinus tracts, dermoids and cystoceles. The acquired causes of TCS are as a result of spinal injury or following surgery for myelomeningocele, or any intradural surgical intervention relevant to the spinal cord8,27,29).
Open surgical detethering of the spinal cord is currently the gold standard and with reported satisfactory postoperative results1,9,13,16,31). However, some patients develop retethering due to scar formation which may require additional surgery24). Recently, minimally invasive surgical techniques have frequently been used for the treatment of spinal pathologies.
The technology of endoscopic spinal surgery has become increasingly popular in recent years due to rapid postoperative recovery and minimal tissue damage4,7,17,18,21). For TCS, although open surgical detethering of the spinal cord is considered to be the gold standard1,9,13,16), endoscopic detethering might also be performed as it is a minimally invasive technique with minimal postoperative discomfort. In the English literature, there are only a few cases of TCS operated on with the endoscopic technique. Here we present a case of TCS operated on with a fully endoscopic surgical technique with special emphasis on the advantages of this approach.
CASE REPORT
1. Case
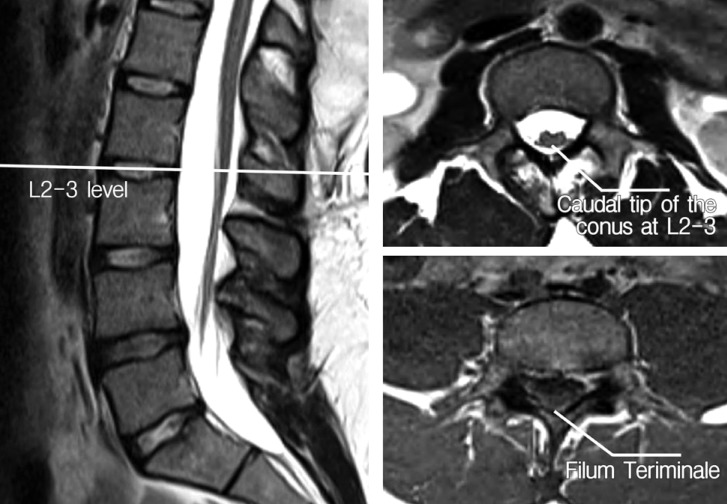
A 19-year-old man was admitted to our neurosurgery clinic with long lasting significant back and bilateral leg pain for which he had undergone several courses of medication and bouts of physical therapy treatment. On examination, he had a lumbosacral hairy dimple and hypoesthesia on the lateral sides of both his thighs. A lumbar magnetic resonance imaging (MRI) scan revealed a thickened, fatty filum with a low-lying conus at the L2-3 level (Fig. 1). The patient's urodynamic parameters were completely normal. Cranial, cervical and thoracic spinal MRI scans were also taken to rule out any associated abnormality. The patient underwent a L4-5 fully endoscopic detethering and sectioning of the fatty filum under electrophysiological monitoring. The procedure resolved his back and leg pain. His hospitalization lasted for only 2 days because of minimal surgical discomfort. At 2-year follow-up, there was no back or leg pain, and his hypoesthesia had resolved completely.
2. Surgical Technique
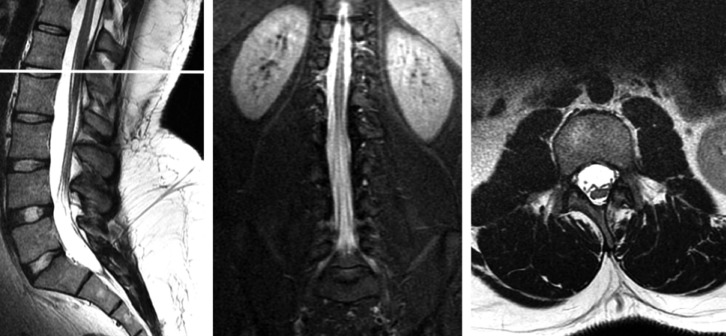
Similar to the relevant literature10), our patient underwent a fully endoscopic detethering of the spinal cord and sectioning of the filum terminale without the assistance of a loupe or microscope. Under general anesthesia, the patient was placed on the operating table in a prone position and an intraoperative lumbar X-ray was used to localize the L4-5 interlaminar window. A 6.9-mm diameter dilator was inserted through a 5-mm skin incision. A 7.9-mm diameter working cannula was inserted onto the ligamentum flavum, then the dilator was removed and the endoscope was inserted. The operation was maintained under direct endoscopic visualization with continuous high-pressure irrigation with physiological serum. With no need for any manipulation of the lamina only through the interlaminar area the ligamentum flavum was removed with the help of micropunches and the dura was exposed. A 5-mm-long dural incision was made with endoscopic scissors. This incision was enlarged and the fatty filum was identified in the dorsal midline. The lower extremities and the anal sphincter were monitored for electromyographic activity. Along with intraoperative neurophysiological monitoring, the thickened filum terminale was located. Controlled stimulation was performed on the L5 and S1 nerve roots to ensure their correct identification. Once stimulation had failed to produce an electromyographic signal from the sphincter, the filum was coagulated using endoscopic radiofrequency and sectioned with endoscopic scissors (Fig. 2). The dura was closed using inlay Duragen and the skin was closed with only one suture owing to the very small skin incision. The operative time required for this procedure was about 45min. In comparative preoperative and postoperative MR images, it was seen that the nerves in the spinal canal were relaxed and there was no cerebrospinal fluid (CSF) leakage (Fig. 3). Two year follow-up MR images showed that conus was elevated and there was no retethering (Fig. 4).
DISCUSSION
Tethered spinal cord syndrome (TCS) is a neurological disorder caused by tissue attachments that limit the movement of the spinal cord by fixing it within the spinal column. The resultant low-lying and immobile conus medullaris leads to spinal cord tension and abnormal stretching of the spinal cord which results in ischemia35).
TCS may be closely associated with spina bifida, lipomeningomyelocele, split cord malformations, dermal sinus tracts, dermoids, and cystoceles. It may also develop after myelomeningocele operations or following any intradural surgical intervention relevant to the spinal cord25,32). Our patient had a lumbosacral hairy dimple, but no history of previous spinal surgery.
In children, TCS may present with lesions, hairy patches, dimples, or fatty tumors on the lower back, foot and spinal deformities, weakness in the legs, change in or abnormal gait including awkwardness while running or wearing the tips or side of one shoe, lower back pain, scoliosis or urinary irregularities26). Adult onset TCS has only been recognized as a definite clinical entity in the past two decades. It is usually diagnosed in childhood, when sensory, motor, bowel, or bladder control issues emerge. This delayed presentation of symptoms relates to the degree of strain on the spinal cord over time. In adults, onset of symptoms typically includes severe leg and/or lower back pain, bilateral muscle weakness and numbness, loss of feeling and movement in the lower extremities, urinary retention, urinary and fecal incontinence3,23,33,34). Our case presented with long lasting significant back and bilateral leg pain and hypoesthesia on the lateral sides of both his thighs.
MRI appears to be the gold standard for diagnosing a tethered cord6). TCS, however, is a clinical diagnosis that should be based on neurological and musculoskeletal signs and symptoms. Imaging features are in general obtained to support rather than make the diagnosis. Aufschnaiter et al.3) emphasized that the conus tip location is not necessarily essential when making the diagnosis of cord tethering. In adults with TCS, the level of the conus tends to be higher than in children20). The level of the conus should therefore not be interpreted in isolation. Tethering can be present with a normally located conus, whereas not every low-lying conus necessarily causes clinical symptoms and requires surgical detethering3,19,32,33). In our case, the diagnosis was made by neurological and musculoskeletal findings and lumbar MRI revealing a fatty filum terminale with low-lying conus at the L2-3 level.
Most authors advocate that surgery should be performed in a timely manner before substantial deficits have evolved20,32,33). Some authors recommend surgery once the diagnosis has been established12), others favor physical therapy as long as the patient responds to it13). Van der Meulen et al.28) reported that early surgery is the most beneficial approach of choice since all of the conservatively followed patients required surgery later and their results were not as good as those who had undergone early surgery. Most of the knowledge with regard to diagnosis, treatment and outcome of TCS is based on experience in children. The benefits and necessity of early surgery in the pediatric group are well-established but the management of adult onset tethered cord syndrome still remains controversial23,30). Our case was an adult patient with TCS who had significant symptoms and who had not benefited from several courses of medication and bouts of physical therapy treatment.
Traditionally, open surgical detethering of the spinal cord has yielded good postoperative results1,9,13,16). However, some patients develop retethering due to intradural scar formation which generally requires additional surgery24). Minimally invasive surgical techniques have been described for the treatment of various spinal pathologies. Endoscopic spinal surgery is a developing field and has had promising surgical results in many areas of spinal surgery. The technology has become increasingly popular in recent years due to rapid postoperative recovery and minimal tissue damage4,7,17,21). However, the use of the endoscope for detethering in TCS is a very new technique covering only a few cases. The technique reported and described by Di10) consists of a 2-cm-long skin incision, hemilaminectomy and use of a retractor with an operative duration of 3 hours. Both techniques (Di's technique and our technique) have the advantages of reduced soft tissue injury, less postoperative pain, minimal blood loss, a smaller incision, and shorter hospitalization. However, unlike Di's technique, ours is a fully endoscopic technique with a 5-mm-long skin incision, a procedure through an interlaminar window with no need for hemilaminectomy, and with an operative duration of only 45 min.
The surgical complication rate is generally low in adult patients11). However, the overall complication rate of 9.5% is within the range of what has previously been reported as 0-12% for tethered cord surgery5,14,15,22). In our case, no complication was encountered.
The incidence of retethering and the indications for repeat surgery remain controversial. In the pediatric age group, Archibeck et al.2) have suggested that retethering is relatively common with 52% of patients in their series requiring revision surgery by the age of 5 years. In contrast, the incidence of retethering in adults seems to be significantly lower. Huttmann et al.15) have reported that, over a mean follow-up period of 8 years, only 16% of patients required repeat detethering surgery. Our patient did not require a repeat detethering procedure during the 2-year follow-up period.
CONCLUSION
Though larger number of cases are needed to make definite conclusions, our technique of fully endoscopic interlaminar detethering of the spinal cord in TCS has the advantages of reduced soft tissue injury, less postoperative pain, minimal blood loss, a smaller incision, and shorter hospitalization. This minimally invasive surgical technique may also provide a decreased likelihood of scar formation and retethering.