INTRODUCTION
C5 palsy is one of the most common postoperative complications after cervical spine decompression surgery. Previously reported rates of C5 palsy after this surgery range from 0% to 30%, and it more commonly affects males3,4,5,11). Nassr et al.9) reported that C5 palsy occurs more frequently in posterior laminectomy and fusion cases than in anterior fusion cases. The time of initial onset of C5 palsy symptoms range from immediately postoperative to 2 months postoperative9). An effective treatment for C5 palsy has yet to be established, but physical therapy aids in joint contracture. With that said, approximately 70% of patients completely recover in 6 months after surgery without treatment, but neurologic deficit remains in approximately 15% of patients9). Bilateral C5 palsy is rare and has been reported to occur in 7% of C5 palsy cases9). But, there has not been any reports describing the onset of palsy symptoms in each of the two sides in bilateral C5 palsy. The etiology of C5 palsy remains unknown, but it is hypothesized that the C5 nerve root is more prone to tethering because it is shorter than other cervical nerve roots.
We report a case of a patient with cervical spondylotic myelopathy who underwent multiple level circumferential fusion and developed bilateral C5 palsy; the right and left sides were afflicted at different postoperative time points. We review the possible factors in the development of this complication.
CASE REPORT
A 61-year-old female had suffered progressive quadriparesis, posterior neck pain, and pain in both arms. Underlying medical diseases included hypertension and end-stage renal disease; she underwent regular hemodialysis. Upon physical examination, her hand grasp muscle strength was grade 3/5 and other extremity strength was grade 4/5. She also had strong positive Hoffmann reflexes on both hands. No differences between her left and right sides were noted.
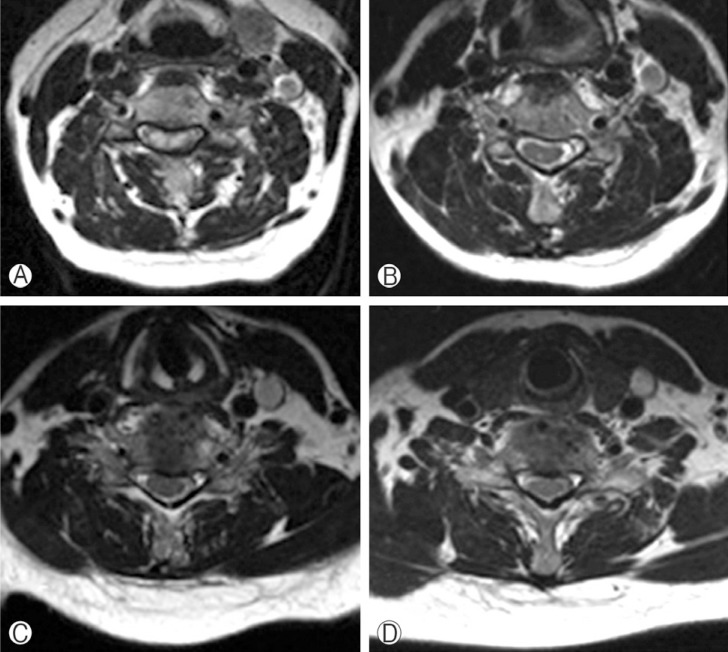
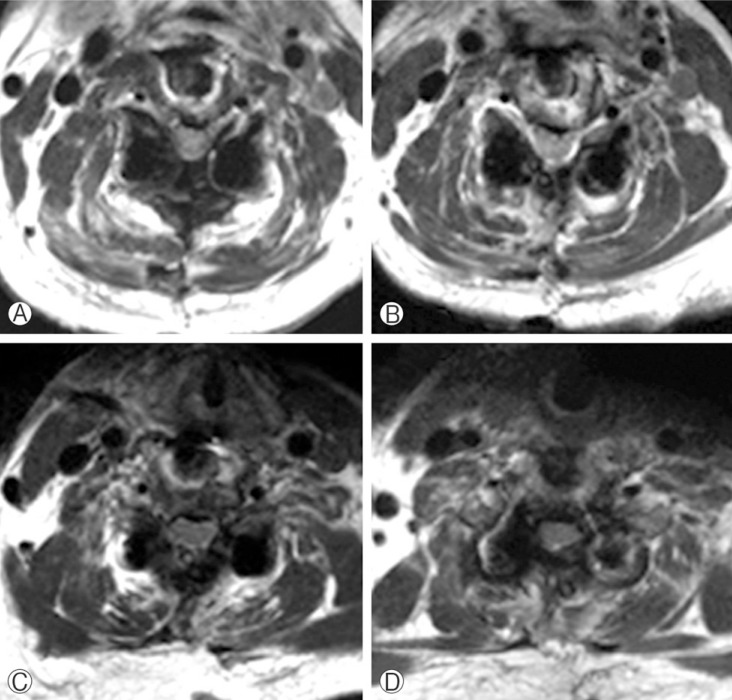
Radiographs of the cervical spine showed multi-level degenerative spondylosis and kyphosis. Preoperative magnetic resonance imaging (MRI) of the cervical spine showed central stenosis on C3/4/5/6/7 and C3/4 spondylolisthesis with a high signal change on the spinal cord (Fig. 1A). Bilateral foraminal stenosis was shown at C3/4 (Fig. 2). She underwent circumferential fusion, which entailed anterior cervical discectomy and fusion of C3-6 using 3 allograft bone blocks inserted at C3-4, C4-5, and C5-6. In addition, total laminectomy at C3-6 and posterior screw fixation at C3-7 was performed. Motor evoked potential (MEP) and somatosensory evoked potential were not done. The surgery was executed gently with microscope. Grossly, no direct nerve root injury was noted during operation. In the recovery room, the patient exhibited no neurologic changes.
On postoperative day (POD) 2, the patient demonstrated weaknesses in her right deltoid and biceps muscles, with a strength grade of 2/5, and had severe pain in her posterior neck and right shoulder. We administered dexamethasone (5mg) intravenously immediately, then every 6 hours for 3 days. Postoperative MRI was performed, and the images showed a mild decrease in spinal cord signals, although screw artifacts could not be ruled out (Fig. 1B, 3). Weakness was only present in the deltoid and biceps muscles on the right side, so we thought that it might be C5 palsy rather than spinal cord edema. She started rehabilitation with electric stimulation and passive exercises.
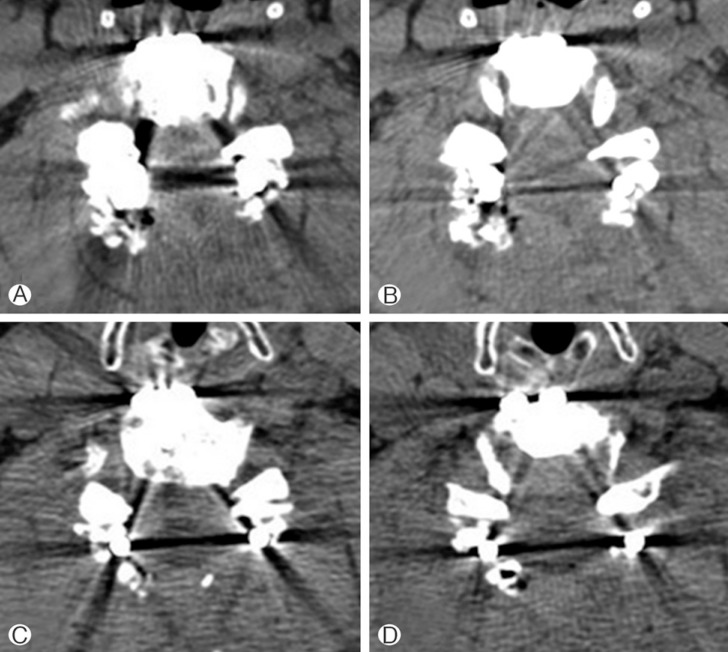
On POD 8, her left deltoid and biceps muscles showed weakness with muscle strength at a grade of 2/5 without neurological changes in other motions. At that time, the patient had mild dysarthria symptoms, so we could not rule out stroke, and we acquired a brain MRI. Brain diffusion MRI showed no signs of a correlative lesion. Cervical spine computed tomography (CT) was performed, and CT showed no newly developed bony lesions or implant problems (screw, rod, or allograft bone) (Fig. 4). Thus, we diagnosed her with bilateral C5 palsy and she continued rehabilitation. At discharge on POD 39, her deltoid and biceps muscles on both the right and left sides had partially recovered to exhibit a muscle strength grade of 3/5. Further improvements were shown in the outpatient department.
DISCUSSION
C5 palsy is a well-known complication of cervical spine decompression surgery. In earlier cases where posterior decompression surgery in the cervical spine was performed, postoperative C5 nerve root palsy was reported. With the development of laminoplasty in the 1980s, several authors reported C5 palsy following the procedure14). C5 palsy presents motor weakness of the deltoid and/or biceps brachii, without myelopathy symptoms. Also, severe pain and sensory deficits can accompany the palsy symptoms5,8).
Many studies have reported that C5 palsy can also be a com plication of anterior cervical discectomy and fusion surgery2). For example, David and Rao reported a case of bilateral C5 motor paralysis following anterior cervical surgery2). The authors concluded that improved lordosis and longitudinal lengthening of the cervical spinal column can paradoxically result in a traction injury to the C5 nerve roots. In addition, Nassr et al.9) reported that, in their sample set, the incidence of C5 palsy was 9.5% for patients undergoing a posterior laminectomy and fusion and 5.1% for patients undergoing an anterior corpectomy.
Recent studies reported that the incidence of C5 palsy after cervical spine decompression surgery ranges from 0% to 30 %4,5,9,11). C5 palsy is typically unilateral but may be bilateral in 5-7% of C5 palsy cases9). The initial onset of symptoms ranges from immediately after surgery to 2 months after surgery9). The exact pathogenesis of C5 palsy remains unknown, but there are several hypotheses: (1) Direct injury to the nerve root during surgical procedure12). For example, the nerve could experience a thermal injury from the high-speed drill; (2) Ischemia and reperfusion injury of the spinal cord1,10); (3) Tethering of the nerve root from shifting of the spinal cord11). The C5 nerve root is uniquely vulnerable to traction injury because it has a few anatomic peculiarities. C5 roots are anatomically located in the center of the cervical lordosis. Also, C5 roots are shorter and follow a more horizontal trajectory than other cervical roots.
The degree of surgical restoration of cervical lordosis may have a bearing on the development of C5 palsy. In our case, because our patient underwent both an anterior and posterior approach, her spinal cord might have become fully decompressed and prone to shifting. Differences between her preoperative and postoperative radiologic images showed a longitudinal expansion of C3-7 vertebrae in terms of height (from 70mm to 83mm), and anterior shifting of the spinal cord approximately 8mm at C5. Moreover, the cervical lordosis (Cobb's angle C3-7) changed -11.8 degrees to +13.8 degrees. As mentioned previously, C5 is at the center of the cervical lordosis, so enough decompression could cause anterior shifting of the spinal cord and cause traction at the C5 nerve root. Also, longitudinal expansion could cause reperfusion injury and edema.
In our case, bilateral C5 palsies were noted at different times postoperatively. We suspect that the palsy symptoms presented at different times due to differences in the severity of compression. Preoperative cervical spine MRI (Fig. 2) showed that the spinal cord was shifted to the right side. Her left C5 root might have been longer because she had been suffering from degenerative cervical spondylosis for a long time, and a longer C5 root could have been bearing traction for a relatively long time. Postoperative cervical spine MRI (Fig. 3) showed that an appropriate amount of decompression had been applied and that the spinal cord had been shifted back to the center. These adjustments might have caused the C5 palsy symptoms to present themselves at different times on the left and right sides. Currently, there is no report on the relationship between the severity of the compression and the onset of C5 palsy symptoms after surgery. Future studies should address this potential association.
Several studies have shown how to both prevent and detect C5 palsies. According to Katsumi et al., postoperative C5 palsy can be avoided by prophylactic bilateral C4/5 foraminotomy7). Also, intraoperative electrophysiology monitoring can be helpful to detect C5 palsies when a decrease in amplitude of the MEP is observed, although this method is not sensitive enough to detect palsies 100% of the time6,13).
Fortunately, over 70% of patients who are afflicted with C5 palsy completely recover9). But, it is important that the surgeon is aware of the possibility of a postoperative C5 nerve root palsy following multilevel decompression surgery in the cervical spine. Decompression can restore the lordotic curvature and height of the cervical spine, but it has the potential to result in a traction injury of C5 nerve roots. Thus, correction of graft height and lordotic curves must be carefully executed to avoid over-traction and resultant complications.
CONCLUSION
Even without direct nerve root injury during an operation, an appropriate amount of decompression can cause traction injury of C5 nerve root. As a complication of cervical spine decompression surgery, C5 palsy can develop unilaterally or bilaterally and the time that elapses between surgery and the onset of symptoms cannot be anticipated. Surgeons should be aware that C5 palsy is always a possible complication of the surgery and must make an effort to prevent possible C5 palsy.