INTRODUCTION
The introduction of microsurgical techniques in 1977 and 1978 by Yasargil20) and Caspar3) represented an important evolution in lumbar disc surgery. Today, microsurgery is considered a standard procedure. However, since the herniated fragment was identified as the offending agent, it has always considered necessary to remove fragment only or the entire disc. This dogma is based on the assumption that increased rates of recurrent disc herniations would follow sequestrectomy alone. For the small subgroup of patients with a free fragment compressing the nerve root, Williams18) was the first to report encouraging results following minimal removal of tissue from the intervertebral disc space. In this subpopulation (≤10% of the overall population with disc herniations), other investigators confirmed success rates of greater than 90% without increased rates of reherniations in retrospective studies5,7,17). Although the recurrence of lumbar disc herniation (LDH) requiring reoperation remains a controversial question in spinal surgery, the incidence of recurrent LDH is reported to linger around 3-13% according to several previous studies14).
The frequency of herniotomy is gradually increasing in LDH treatment. Herniotomy used to be synonymous with fragmentectomy or sequestrectomy. The term 'herniotomy' is defined as removal of the herniated disc fragment only, and the 'conventional discectomy' as removal of the herniated disc and degenerative nucleus from the intervertebral disc space. This study compared herniotomy with conventional discectomy by examining the rate of recurrent disc herniation requiring revision surgery after herniotomy. Furthermore we discussed the radiologic indications of herniotomy and analyzed differences in two procedures by comparing with the clinical outcome of conventional discectomy.
MATERIALS AND METHODS
This study is a retrospective case control study performed from June 2009 to May 2012 on single-level LDH patients. Information was gathered from the medical chart, radiologic review, and telephone interview. During three years, 57 patients underwent herniotomy by a single surgeon. 631 patients were received conventional discectomy during the same period of experimental group by the same surgeon. To minimize the biases of surgeons, we selected 57 patients as a control group who received conventional discectomy by the same surgeon. Subjects in the control group were selected using a random number generator while considering the sex and age of patients for efficiency of the study. This study protocol was reviewed and approved by our Institutional Review Board. In first postoperative week of the initial follow-up period, the postoperative VAS and the Korean version of ODI were examined. Subsequently, subjects' clinical outcomes were investigated based on Odom's criteria6) every three month for three years. Data were analyzed by independent t-test and Fisher's exact test. Null hypotheses of no difference were rejected if p-values were less than .05. SPSS 18.0 (SPSS, Inc, Chicago, IL) was used for statistical analysis.
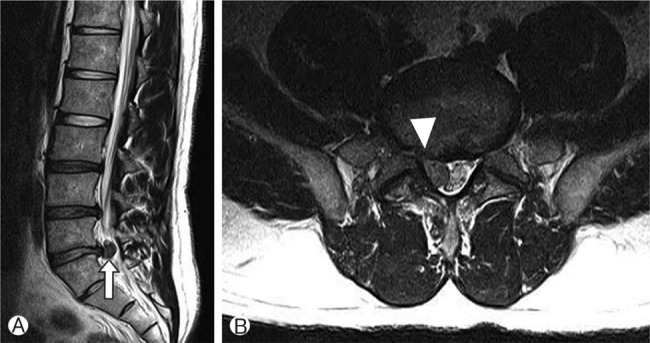
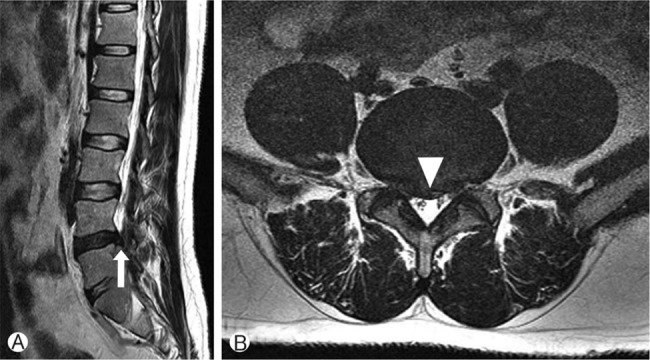
Recurrent LDH was defined as a condition of reoperative sign and symptom after removal of primary lesion in immediate postoperative MR, followed by pathologic confirmation of disc herniation on enhanced MR images. We always carried out postoperative MR on 3rd or 4th day after surgery. So the patient that had remnant disc was excluded in this study. Reoperative sign and symptom meant that patient showed almost same condition before surgery. At that time, we rechecked MR. And we compared with rechecked MR to baseline MR. The study established the radiologic indications of herniotomy as detection of free fragment on MR scan, low continuity with disc spaces, and minimal disc protrusion of parent disc (Fig. 1). In contrast, the patient with less continuity with disc space and wide disc protrusion in MR scan underwent conventional discectomy (Fig. 2). However, the final confirmation of herniotomy was decided based on intraoperative findings.
RESULTS
Among 114 single-level LDH patients, level L4-5 was the most common level, as already known, for disc herniation in herniotomy and discectomy, followed by two levels L5-S1 and L3-4 (Table 1). We found 57 patients undergoing herniotomy and selected 57 patients undergoing conventional discectomy considering age and gender. The male to female ratios were 33:24 in herniotomy group and 31:26 in conventional discectomy group. The average ages were 50 years old in the herniotomy group and 47.6 years old in the conventional discectomy group.
There were four cases (7%) of recurrence in the herniotomy group and three (5.7%) in the discectomy group. Although the herniotomy group had one more case of recurrence, this was not a significant difference (p=1.000). Recurrence levels ranked in the order of common cases and the average recurrent intervals were 16.5 weeks in herniotomy and 29 weeks in conventional discectomy groups (Table 2).
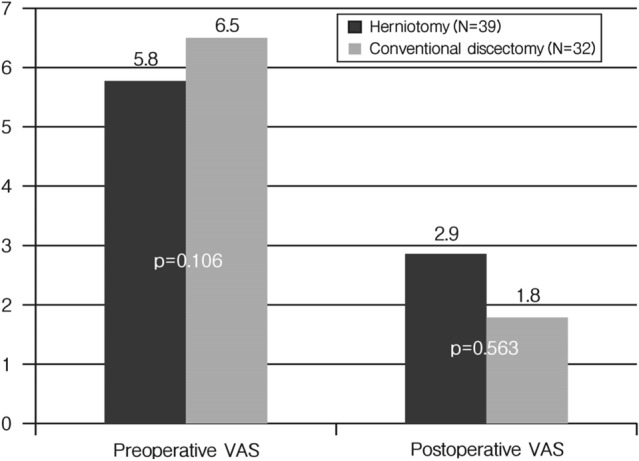
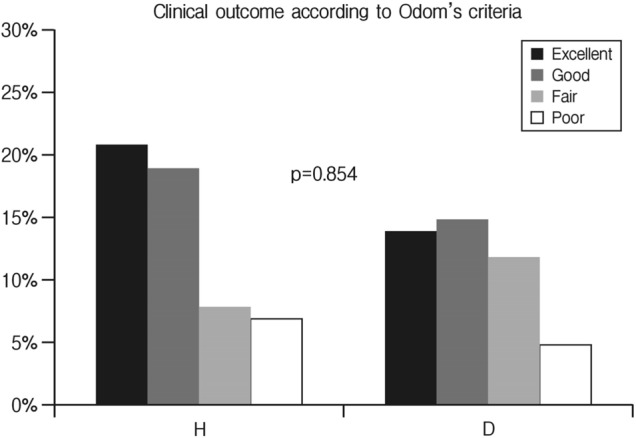
The VAS and Korean version of ODI of several people were unobtainable due to some data about VAS and ODI was not filled in chart. The VAS was obtained before and one week after surgery. So among the 57 subjects, 39 patients in herniotomy group and 32 patients in conventional discectomy group participated in a survey. The pre and postoperative VAS decreased from 5.8 to 2.9 points in the herniotomy group and from 6.5 to 1.8 points in the discectomy group, a greater decrease in VAS compared to the herniotomy group (Fig. 3). In Korean version of ODI, the preoperative score of 45.87 decreased to a postoperative score of 25.44 in herniotomy group. In conventional discectomy group, the preoperative score of 48.33 decreased to the postoperative score of 28.64. Both groups showed similar levels of decrease (Fig. 4). However, no significant differences were found in VAS and Korean version of ODI outcomes between two groups (Table 3). The average follow-up period was 1.2 years when patients' conditions were confirmed through telephone interview between three months and three years postoperatively. Also results were classified based on Odom's criteria. Excellent indicated all preoperative symptoms relieved and abnormal findings improved. Good indicated minimal persistence of preoperative symptoms and abnormal findings unchanged or improved. Fair indicated definite relief of some preoperative symptoms and other symptoms unchanged or slightly improved. Poor indicated symptoms and signs unchanged or exacerbated. A telephone interview survey was administered to 32 out of 57 patients in the herniotomy group and 27 out of 57 patients in the discectomy group. This survey found 37.5% answered excellent and 34.4%patients good in the herniotomy group. Similarly, 29.7% patients answered excellent and 33.3% good in discectomy group (Table 4). There was no significant difference (p-value between the two groups according to the criteria was 0.854. p-value in Excellent+Good vs. Fair+Poor was 0.517. Excellent vs. the others was 0.781) (Fig. 5).
DISCUSSION
We have described the results of the retrospective case control study for comparison of early and three years outcome after herniotomy and conventional discectomy in 114 patients with herniated lumbar discs. The repeated operation rate did not increase following removal of the herniated material only in our study. Traditionally, microdiscectomy-related neural decompression was achieved by excision of the herniated disc material, resection of as much intervertebral tissue as possible, and curettage of the endplates2). This technique has been based on the assumption that the likelihood of reherniation would be reduced by increasing the amount of resected disc tissue17). This dogma has hardly been challenged, although scientific evidence justifying it is lacking. Complete removal of all disc material is impossible9,12). Consequently, repeated operations could not be avoided when this approach has been used3,5). On the other hand, aggressive discectomy has been associated with reduced intervertebral height, which is thought to cause segmental instability and thus accelerate spondylosis4,8,10). This may contribute to the significant risk of failed-back surgery syndrome as well as late-onset sequelae of disc surgery after asymptomatic intervals. Although long-term studies for evaluating these sequelae are scarce, some investigators have shown that the prevalence of low-back pain in patients who do not undergo endplate curettage is reduced1). Mochida et al.13) confirmed that less aggressive removal of disc material might be associated with better radiographic and clinical results. Williams18,19) introduced the concept of microsurgical removal of the offending material resulting in minimal injury to the surrounding osseous, articular, and disc structures. His technique includeed dilation of the anulus fibrosus, excision of tissue fragments "which can be easily mobilized from the intervertebral space," and visualization of the nerve root. He reported recurrence rates of 4 to 9% and a clinical success rate of 90%. Several investigators have confirmed these results7,16,17), which have been thoroughly summarized by Wenger et al.17) The results compare favorably with those achieved after microdiscectomy (recurrence rates 3-11%; clinical success rates 50-90%). Rogers15), however, reported a recurrence rate of 21% (seven of 33 patients) after excision of only the herniated fragments. Unfortunately, these studies are retrospective and lack an adequate control group, thus limiting scientific power. An additional advantage of herniotomy is that abdominal or retroperitoneal injury is avoided because the disc space is not entered. Although extremely rare, these complications have been associated with devastating results8). In his 12-year review, however, Williams19) reported that 92% of reherniations occurred within the first9) months, and Rogers15) indicated that most recurrences appeared within 6 months. In this study, the reoperation rate of 5.2% after conventional discectomy (three of 57 patients) seems similar to the literature. Reherniation in 7% of herniotomy treated patients is in accordance with the literature17). Regardless of the necessity for longer follow-up review, we believe that our findings provide some evidence that reherniations are not increased after herniotomy. It is interesting that the mean time to recurrence was nearly double in the conventional discectomy group (29 weeks versus 16.5 weeks). But there is no necessity to give a meaning because the number of recurrent patients was too small. The postoperative VAS of conventional discectomy patients group decreased more than herniotomy group. This result may be because the postoperative VAS was checked one week after surgery. There is no significant difference in VAS between groups. Also, clinical outcomes according Odom's criteria show less satisfaction as usual11). However, we expect that long-term VAS and clinical outcomes will show a better result in herniotomy group.